When you have a high profile passenger killed with lots of press interest, one of two things are sure to happen in the investigation. If it was a military mishap, the cause will be found and ignored if necessary to point blame at the military. If it was a civilian mishap and the cause points to a company with powerful friends in Washington, D.C., the cause will be ignored if necessary and the blame will be undetermined. This is a case of the latter.
— James Albright

Updated:
2015-07-11
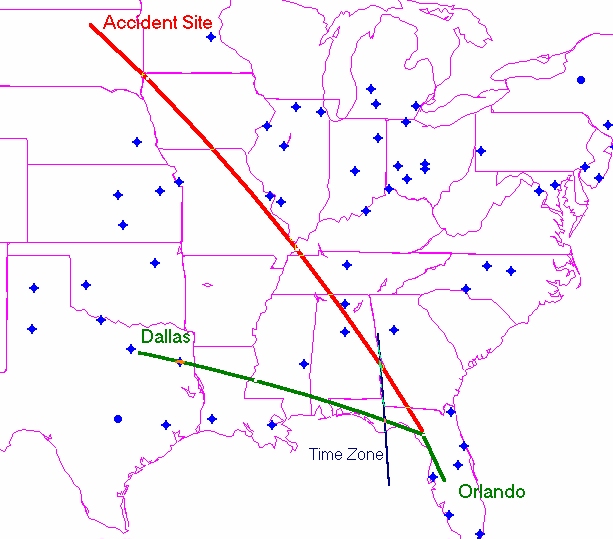
NTSB-N47BA Slide 0046,
from NTSB Slide Show
The aircraft failed to pressurize or lost pressurization for unknown reasons. The crew failed to receive supplemental oxygen for unknown reasons. When I was an Air Force safety officer, we were told that while the criminal and legal investigators needed to find evidence "beyond a reasonable doubt," our criteria was, simply, it had to be reasonable. We were in the business of preventing future mishaps, after all. Reading the accident report and examining the accident docket, I believe the following are reasonable conclusions:
- Sunjet Aviation failed to service the oxygen system for nearly two months. A company official stated the captain reported the oxygen pressure was in the green zone the day of the accident. I find it highly unlikely that the captain would report this fact to anyone. The captain should have checked it. And if he did, he would more likely simply note the fact and move on. I think it much more likely that the company failed to service the oxygen all that time and the captain failed to check it.
- The aircraft out-climbed the pressurization system. The pressurization system had a history of inflow problems but no history of pressure vessel leaks. The NTSB looked at the nearly closed bleed air valves and assumed this meant the inflow was keeping up with the leak rate and was providing sufficient air. This faulty logic ignores the fact the aircraft wasn't adequately pressurized so either the air input was inadequate or the output was excessive. Given the history of the airplane's input system, they should not have dismissed this so quickly.
- The crew suffered from slow onset hypoxia. The most dangerous form of hypoxia comes from a gradual increase, studies indicate that about 1,500 fpm being the most insidious. It could very well be that they became partially hypoxic during the climb. The last communication was as the aircraft passed 23,200 feet. Perhaps the cabin had not yet exceeded 10,000 feet when the aural warning would have sounded. When that happened they may have donned their masks but didn't receive any oxygen because the tank was empty. They were mentally impaired and rather than descend they attempted to troubleshoot.
Yes, this is speculation. So regardless if you choose to believe this scenario or not, there are several lessons we can take away from this mishap:
- Fuselage pressure leaks should be addressed immediately and repaired.
- Oxygen supply and delivery equipment must be pre-flighted.
- During every climb, part of your 10,000 foot check must be a check of cabin altitude. Most airplanes have a maximum cabin altitude between 6,000 and 8,000 feet. You certainly should not be above that at 10,000 feet aircraft altitude. You should know your normal cabin climb rate, typically around 300 fpm. Even if it takes you ten minutes to get to 10,000 feet aircraft altitude, you should not see more than 3,000 feet cabin altitude at that point. In any case, if it isn't where it should be, level off and investigate.
- When troubleshooting a pressurization problem, donning oxygen quickly will not only improve your mental capabilities, it can keep you in the game if things go south quickly or insidiously.
- When in doubt, descend.
The lesson here for us pilots may not be as obvious as you think, especially given the NTSB pronouncement that the pilots were incapacitated because of "their failure to receive supplemental oxygen following a loss of cabin pressurization, for undetermined reasons." So let me spell it out: if you are flying for an organization that is prone to cutting corners, you should double your efforts to do everything by the book.

1
Accident report
- Date: 25 OCT 1999
- Time: 12:13 CDT
- Type: Learjet 35A
- Operator: Sunjet Aviation
- Registration: N47BA
- Fatalities: 2 of 2 crew, 6 of 6 passengers
- Aircraft Fate: Destroyed
- Phase: En route
- Airports: (Departure) Orlando International Airport, FL (MCO/KMCO), United States of America; (Destination) Dallas-Love Field, TX (DAL/KDAL), United States of America
2
Narrative
- According to ATC radio transmissions, the flight departed MCO about 0919 EDT bound for DAL. At 0921:46 EDT, the flight contacted the Jacksonville Air Route Traffic Control Center (ARTCC) and reported climbing through an altitude of 9,500 feet to 14,000 feet.
- At 0921:51 EDT, the controller instructed N47BA to climb and maintain FL 260. N47BA acknowledged the clearance by stating, “two six zero bravo alpha.” At 0923:16 EDT, the controller cleared N47BA direct to Cross City and then direct to DAL. N47BA acknowledged the clearance. At 0926:48 EDT, N47BA was issued instructions to change radio frequency and contact another Jacksonville ARTCC controller. N47BA acknowledged the frequency change.
- At 0927:10 EDT, N47BA called the Jacksonville ARTCC controller and stated that the flight was climbing through an altitude of FL 230. At 0927:13 EDT, the controller instructed N47BA to climb and maintain FL 390. At 0927:18 EDT, N47BA acknowledged the clearance by stating, “three nine zero bravo alpha.” This was the last known radio transmission from the airplane. The sound of the cabin altitude aural warning was not heard on the ATC recording of this transmission.
- At 0933:38 EDT (6 minutes and 20 seconds after N47BA acknowledged the previous clearance), the controller instructed N47BA to change radio frequencies and contact another Jacksonville ARTCC controller. The controller received no response from N47BA. The controller called the flight five more times over the next 4 1/2 minutes but received no response.
- About 0952 CDT, a USAF F-16 test pilot from the 40th Flight Test Squadron at Eglin Air Force Base (AFB), Florida, was vectored to within 8 nm of N47BA. About 0954 CDT, at a range of 2,000 feet from the accident airplane and an altitude of about 46,400 feet, the test pilot made two radio calls to N47BA but did not receive a response. About 1000 CDT, the test pilot began a visual inspection of N47BA. There was no visible damage to the airplane, and he did not see ice accumulation on the exterior of the airplane. Both engines were running, and the rotating beacon was on. He stated that he could not see inside the passenger section of the airplane because the windows seemed to be dark. Further, he stated that the entire right cockpit windshield was opaque, as if condensation or ice covered the inside. He also indicated that the left cockpit windshield was opaque, although several sections of the center of the windshield seemed to be only thinly covered by condensation or ice; a small rectangular section of the windshield was clear, with only a small section of the glare shield visible through this area. He did not see any flight control movement. About 1012 CDT, he concluded his inspection of N47BA and proceeded to Scott AFB, Illinois.
- About 1113 CDT, two Oklahoma ANG F-16s with the identification “TULSA 13 flight” were vectored to intercept the accident airplane by the Minneapolis ARTCC. The TULSA 13 lead pilot reported to the Minneapolis ARTCC controller that he could not see any movement in the cockpit. About 1125 CDT, the TULSA 13 lead pilot reported that the windshield was dark and that he could not tell if the windshield was iced.
- About 1133 CDT, a TULSA 13 airplane maneuvered in front of the accident airplane, and the pilot reported, “we’re not seeing anything inside, could be just a dark cockpit though . . . he is not reacting, moving or anything like that he should be able to have seen us by now.”
- About 1138 CDT, the TULSA 13 lead pilot stated, “my wingman is going to make a final pass and then we are going to head back to the [midair refueling] tanker.” The TULSA 13 wingman reported, “we did not get close enough to see any icing on the window due to our configuration...we did get up behind him but did not see anything.” About 1139 CDT, TULSA 13 flight departed for the tanker.
- About 1150 CDT, two North Dakota ANG F-16s with the identification “NODAK 32 flight” were vectored to intercept N47BA. (TULSA 13 flight had returned from refueling, and both TULSA 13 and NODAK 32 flights maneuvered in close proximity to N47BA.) About 1157 CDT, the TULSA 13 lead pilot reported, “we’ve got two visuals on it. It’s looking like the cockpit window is iced over and there’s no displacement in any of the control surfaces as far as the ailerons or trims.” About 1201 CDT, TULSA 13 flight returned to the tanker again.
- At 1210:41 CDT, the sound of an engine winding down, followed by sounds similar to a stickshaker and an autopilot disconnect, can be heard on N47BA’s cockpit voice recorder (CVR), which recorded the final 30 minutes of cruise flight. The CVR also captured the continuous activation of the cabin altitude aural warning, which ceased at 1212:26 CDT. At 1211:01 CDT, ATC radar indicated that N47BA began a right turn and descent. One NODAK 32 airplane remained to the west, while one TULSA 13 airplane broke away from the tanker and followed N47BA down. At 1211:26 CDT, the NODAK 32 lead pilot reported, “the target is descending and he is doing multiple aileron rolls, looks like he’s out of control . . . in a severe descent, request an emergency descent to follow target.” The TULSA 13 pilot reported, “It’s soon to impact the ground he is in a descending spiral.”
Source: NTSB Aircraft Accident Brief, AAB-00/01, page 2
3
Analysis
- The captain was hired by Sunjet Aviation on September 21, 1999. According to Sunjet Aviation records, the captain had accumulated a total of 4,280 hours of flight time (including his military flight time). He had flown a total of 60 hours with Sunjet Aviation, 38 hours as a Learjet pilot-in-command and 22 hours as a Learjet second-in-command. The captain had flown 35 and 6 hours in the last 30 and 7 days (respectively) and 0 hours in the last 24 hours before the accident. Sunjet Aviation records indicate that the captain received his initial Learjet 35 type rating and completed the airman competency/proficiency check for the Learjet 35 on September 21, 1999. According to Sunjet Aviation employees, the captain was an excellent pilot who transitioned into the Learjet without difficulty. They also indicated that he was knowledgeable about the airplane and that he was a confident pilot with good situational awareness.
- The first officer was hired by Sunjet Aviation on February 24, 1999. According to Sunjet Aviation records, the first officer had accumulated a total of 1,751 hours of flight time, 1,300 of which were as a pilot-in-command. She had flown a total of 251 hours with Sunjet Aviation as a second-in-command, 99 hours of which were as a Learjet second-in-command. The first officer had flown 35 and 6 hours in the last 30 and 7 days (respectively) and 0 hours in the last 24 hours before the accident. Sunjet Aviation records indicate that the first officer received her initial Learjet 35 type rating, completed her initial Learjet 35 second-in-command check ride, and completed the airman competency/proficiency check for the Learjet 35 on April 15, 1999. Pilots who had flown with the first officer before she was hired by Sunjet Aviation indicated that she was a knowledgeable pilot with good aircraft handling skills; one pilot stated that she was a serious pilot who had a “meticulous” style in the cockpit and was not someone who abbreviated procedures or neglected checklists. Sunjet Aviation pilots indicated that she was a confident pilot with excellent radio communication skills.
Source: NTSB Aircraft Accident Brief, AAB-00/01, page 5
- The flight crew’s last communication with air traffic control (ATC) was at 0927:18 eastern daylight time, when the first officer acknowledged an ATC clearance to flight level (FL) 390 and the airplane was climbing through 23,200 feet. Her speech was normal, her phraseology was accurate and appropriate, and Safety Board testing indicated that she was not using an oxygen mask microphone for this transmission or those that she had made earlier. The flight crew’s failure to respond to repeated ATC radio inquiries beginning at 0933:38, when the airplane was climbing through about 36,400 feet, was the first indication of a problem on board the accident flight. As the flight continued, it deviated from its assigned course and failed to level at its assigned altitude (FL 390).
- The continuous sounding of the cabin altitude aural warning during the final 30 minutes of cruise flight (the only portion recorded by the CVR) indicates that the airplane and its occupants experienced a loss of cabin pressurization some time earlier in the flight. Further, although the severity of the impact precluded extensive analysis, there was no evidence suggesting any alternative reason for incapacitation.
- If the pilots had received supplemental oxygen from the airplane’s emergency oxygen system, they likely would have properly responded to the depressurization by descending the airplane to a safe altitude. Therefore, it appears that the partial pressure of oxygen in the cabin after the depressurization was insufficient for the flight crew to maintain consciousness and that the flight crewmembers did not receive any, or adequate, supplemental oxygen.
- Post accident examination of the left and right bleed air shutoff/regulator valves (modulation valves) indicated that they were near their fully closed positions. Because the modulation valves are spring loaded to the open position and require bleed air to close, the nearly closed position of both valves at impact is consistent with a normal and adequate supply of engine bleed air from one or both engines. Further, these nearly closed valve positions indicate that there was a low demand for bleed air by the airplane’s air conditioning and anti-icing systems and that both BLEED AIR switches, which were not recovered, would have had to have been selected to the ON position. The nearly closed valve positions also indicate that the airplane’s pneumatic system was intact, and, therefore, normal system pressure was being supplied to the air conditioning system flow control valve.
Source: NTSB Aircraft Accident Brief, AAB-00/01, page 27
This is faulty logic. If the aircraft was normally pressurized, these valves would indeed be nearly closed. But the aircraft was not normally pressurized and the fact these valves were nearly closed is a major clue. Either not enough air was going in or too much was going out. The airplane had a history of air inflow problems.
- The flow control valve regulates the flow rate of conditioned bleed air entering the cabin for pressurization and heating. If there is no inlet bleed air, the valve main spring will close the flow control valve completely. Although, as previously discussed, bleed air was available to open the flow control valve, the condition of the flow control valve indicated that it was in its fully closed position at impact. The valve requires several seconds to move from its fully open to fully closed position in normal operation, indicating that the valve was in its closed position before impact. This closed valve would have prevented bleed air from entering the cabin, thereby preventing normal pressurization.
- Closure of the flow control valve on a Learjet Model 35 and the resulting loss of bleed air supply to the cabin would cause the airplane to quickly lose cabin pressure (depressurize) at a rate dependent upon the cabin leakage rate. Computer simulations by Honeywell indicated that if a loss of normal bleed air supply to the cabin occurred at flight altitudes above 25,000 feet, the cabin altitude could ascend to 10,000 feet in about 30 seconds and reach 25,000 feet in about 2 1/2 minutes.
Source: NTSB Aircraft Accident Brief, AAB-00/01, page 27
That is a pretty rapid rate, hard to miss. It is hard to imagine the flow control valve was operating normally and then suddenly closed without getting someone's attention.
- Investigators also considered the possibility that the pilots failed to select the CABIN AIR switch to NORM, which activates the air conditioning system (and pressurizes the airplane), before takeoff. Even though the Taxi and Before Takeoff checklist specifies, in item 19, “CABIN AIR SWITCH - NORM,” the FAA Special Certification Review (SCR) team observed that “there is incentive to leave the pressurization system off during taxi and takeoff in warm weather because inflow air can be hotter than cabin ambient air.” However, without the cabin air conditioning system, the occupants of the airplane likely would have perceived a high cabin climb rate after takeoff, possibly causing discomfort. At about 10,000 feet cabin altitude, the cabin altitude aural warning should have begun to sound, further alerting the flight crew to the lack of pressurization. Although the pilots could have manually silenced the warning, they would have had to repeat this action every 60 seconds. At about 14,000 feet cabin altitude, deployment of the passengers’ oxygen masks would have provided an additional cue that the cabin was not properly pressurized. It is unlikely that the flight crew would have continued to climb despite this clear information that the airplane was unpressurized.
- In summary, as previously discussed, an uncommanded closure of the flow control valve would have been sufficient to depressurize the airplane. However, there was insufficient evidence to determine whether the depressurization was initiated by a loss of bleed air inflow (caused by a malfunction of the flow control valve or by inappropriate or incomplete flight crew action) or by some other event.
Source: NTSB Aircraft Accident Brief, AAB-00/01, page 27
It is unclear why the airplane failed to properly pressurize, but the preponderance of evidence points to a lack of inflow air.
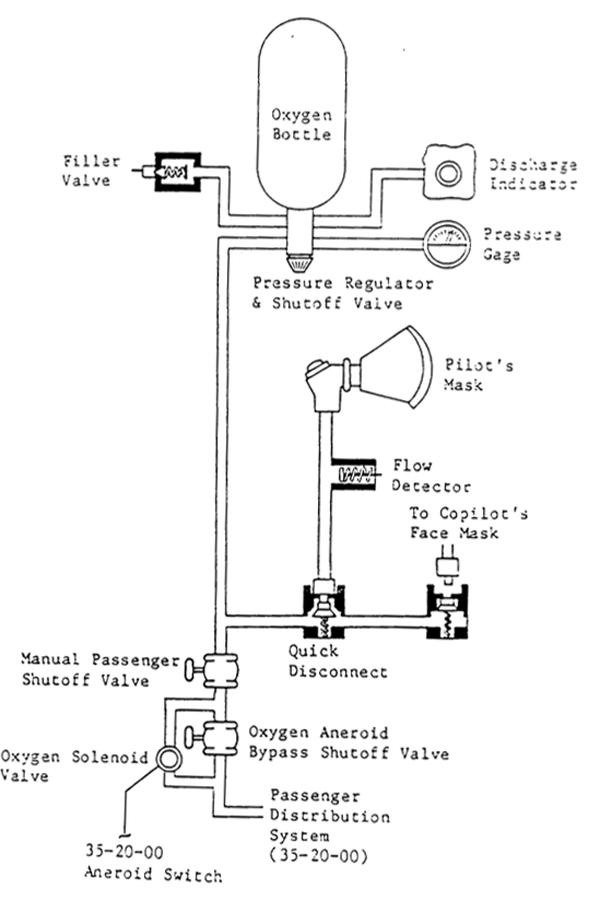
LR-35 Crew Oxygen System Schematic,
from NTSB DCA00MA005
Following the depressurization, the pilots did not receive supplemental oxygen in sufficient time and/or adequate concentration to avoid hypoxia and incapacitation. The wreckage indicated that the oxygen bottle pressure regulator/shutoff valve was open on the accident flight. Further, although one flight crew mask hose connector was found in the wreckage disconnected from its valve receptacle (the other connector was not recovered), damage to the recovered connector and both receptacles was consistent with both flight crew masks having been connected to the airplane’s oxygen supply lines at the time of impact. In addition, both flight crew mask microphones were found plugged in to their respective crew microphone jacks. Therefore, assuming the oxygen bottle contained an adequate supply of oxygen, supplemental oxygen should have been available to both pilots’ oxygen masks.
Source: NTSB Brief, AAB-00/01, page 32
There was a lot of speculation in the Learjet world about the position of the oxygen system pressure regulator and shutoff valve, reasoning that many operators shut the valve off between flights to prevent system leakage. The valve was found in the open position and this operator did not, as a practice, close the valve.
- The sequence of maintenance actions from July 22 through October 23, 1999, indicate that there were several pressurization-related discrepancies during this period. Maintenance records indicate that Sunjet Aviation personnel attempted to correct the discrepancies by cleaning the pressurization system outflow valve and performing system ground checks. Work on a staggered engine throttle condition, which resulted in the replacement of the left modulation valve on October 23, 1999, was also related to concerns about the pressurization system (as shown by Sunjet Aviation’s reference to pressurization on the removed modulation valve’s part tag). However, Sunjet Aviation was not able to provide records of pilot-reported discrepancies that led to these maintenance actions.
- The airplane’s maintenance records indicate that the oxygen bottle was last serviced with oxygen (by Sunjet Aviation) on September 3, 1999.
Source: NTSB Brief, AAB-00/01, page 31
That is nearly two months prior to the mishap flight.
- A Sunjet Aviation official stated to the Safety Board that the accident captain had reported that the oxygen pressure gauge was in the green zone, indicating adequate pressure of 1,550 to 1,850 psi, during preflight checks on the day of the accident.
Source: NTSB Brief, AAB-00/01, page 31
This appears to me to be fully fabricated, a way of covering up the fact the oxygen had not been serviced in nearly two months. I have never reported that a required item was in the normal zone to any official following my aircraft preflight. I have, many times, reported that the oxygen was insufficient and asked that it be serviced. But why would any pilot report the oxygen is okay in this situation?
- The Safety Board contacted fixed-based operators (FBO) at 15 known destination airports visited by the accident airplane between September 26 and October 20, 1999, and none had any record of charges for oxygen servicing of the accident airplane. However, the Board cannot exclude the possibility that the airplane was serviced with oxygen after September 3, 1999, at a different airport or at no charge to Sunjet Aviation61 and that no record was made.
- In summary, the Safety Board could not determine the quantity of oxygen that was on board the accident flight.
Source: NTSB Brief, AAB-00/01, page 31
- Investigations of other accidents in which flight crews attempted to diagnose a pressurization problem or initiate emergency pressurization instead of immediately donning oxygen masks following a cabin altitude alert have revealed that, even with a relatively gradual rate of depressurization, pilots have rapidly lost cognitive or motor abilities to effectively troubleshoot the problem or don their masks shortly thereafter. In this accident, the flight crew’s failure to obtain supplemental oxygen in time to avoid incapacitation could be explained by a delay in donning oxygen masks of only a few seconds in the case of an explosive or rapid decompression or a slightly longer delay in the case of a gradual decompression.
Source: NTSB Brief, AAB-00/01, page 35
4
Cause
The National Transportation Safety Board determines the probable cause of this accident was incapacitation of the flight crewmembers as a result of their failure to receive supplemental oxygen following a loss of cabin pressurization, for undetermined reasons.
Source: NTSB Brief, AAB-00/01, page 35
References
(Source material)
NTSB Aircraft Accident Brief, AAB-00/01, DCA00MA005, Sunjet Aviation, Learjet Model 35, N47BA, Aberdeen, South Dakota, October 25, 1999