This case study speaks for itself, there are a lot of lessons to be learned for pilots who are confident, perhaps overconfident, in their abilities.
— James Albright

Updated:
2018-10-12


1
Accident report
- Date: 14 FEB 2011
- Time: 1315
- Type: Gulfstream G550
- Operator: Gulfstream Aerospace Corporation
- Registration: N535GA
- Fatalities: 0 of 2 crew, 0 of 1 passengers
- Aircraft Fate: Substantially damaged
- Phase: Landing
- Airports: (Departure) Outagamie County Regional Airport, WI (ATW/KATW), United States of America; (Destination) Outagamie County Regional Airport, WI (ATW/KATW), United States of America
2
Narrative
The Gulfstream G550 has two primary hydraulic systems: the bulk of the airplane, including flight controls, is operated by the left system and critical flight control systems are backed up by the right system. Because so much is on the left system, there are multiple back ups. The wheel brakes are normally powered by the left system. If the left system pumps go bad, the right system can provide pressure using left system quantity. If left system quantity is depleted, an auxiliary system can power the brakes, depending on where the left system leak is. If all left system quantity is gone, a brake accumulator can provide emergency braking.
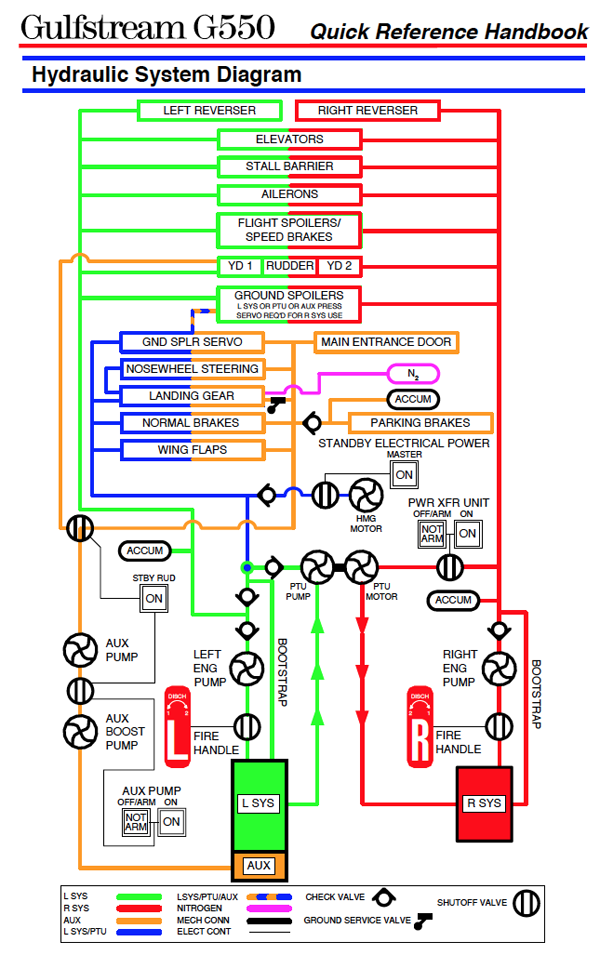
G550 Hydraulic System Schematic, from G550 Quick Reference Handbook, pg. EE-2.
- On February 14, 2011, about 1315 central standard time, a Gulfstream Aerospace Corporation GV-SP airplane, N535GA, had a landing overrun on runway 30 (6,501 feet by 150 feet, dry grooved concrete) at the Outagamie County Regional Airport (ATW), near Appleton, Wisconsin, following a reported loss of a hydraulic system. The two airline transport pilots and one passenger were not injured. The airplane incurred substantial left wing damage when the left main landing gear collapsed during the overrun.
- The airplane was registered to and operated by Gulfstream Aerospace Corporation under the provisions of 14 Code of Federal Regulations Part 91 as a maintenance test flight.
- Day, visual flight rules conditions prevailed for the flight, which operated on an activated instrument flight rules flight plan. The local flight departed from ATW about 1010.
- According to the report submitted by the operator, a preflight brief started at 0815 and some "write ups" were noted. Taxi, engine "run-ups", and takeoff were reported as normal. The flight to the Marquette, Michigan, area was normal. All inflight checks were found to be normal. However, write ups were noted with the number one flight management system, the elevator trim, and Mach trim. The autopilot disengaged during two inflight maneuvers. Following a low approach at the Austin Straubel International Airport, near Green Bay, Wisconsin, the flight crew was cleared direct to SUDIE, an initial approach fix for the area navigation (RNAV)/global positioning system (GPS) runway 30 approach at ATW.
- Flaps 10 degrees were selected prior to an intermediate fix named "APESE." Flaps 20 degrees were selected between APESE and the final approach fix (FAF) named "ZUMUG." A discussion about another approach and maintenance issues was conducted and a full stop landing was decided upon to follow the GPS approach. As the airplane approached the virtual glide slope, the pilot flying (PF) called for the landing gear to be selected down and called for the landing checklist to be conducted. The landing gear came down with an indication of three green lights and no red lights. The pilot not flying (PNF) completed the before landing checklist to "include arming ground spoilers, warning inhibit, pumping up Brakes/Hydraulics/Brake Accumulator to 3000 psi" except for "selecting full flaps." Full flaps were to be selected at the PF's call for full flaps. The PNF also selected the Landing Mode on the Cabin Pressure Controller. Subsequent to that, an amber left side hydraulic quantity low crew alerting system (CAS) message illuminated when the airplane was inside the FAF.
Source: NTSB Factual Report, pg. 1
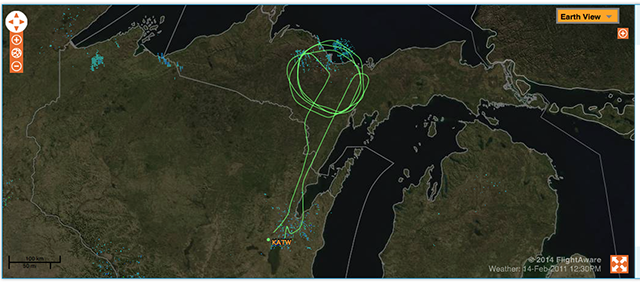
N535GA Route of Flight, from flightware.com
- The PF selected the hydraulic synoptic page and noticed the hydraulic quantity decreasing. The PF called for flaps full and PNF selected flaps full. No movement of the flaps occurred so the PNF re-selected flaps 20 degrees. Shortly after that an amber left hydraulic system fail CAS message appeared. The PNF pulled out the checklist to accomplish the procedures related to the left hydraulic system fail CAS message and suggested a go-around. At the beginning of the checklist, there is a note that, in part, indicated, "Select a runway that is at least 7,000 feet (2133.6 m) long and 150 feet (45.7 m) wide." According to the operator's report, the PF decided to land due to the significant hydraulic leak and the airplane was in a landing configuration below 1,000 feet above ground level (AGL) with prior autopilot/trim problems.
Source: NTSB Factual Report, pg. 1

13:12:17.8 HOT-2 — should we go around to check it out?
13:12:19.5 HOT-1 — no . . . we're gonna land cause it's leakin'
13:12:20.8 HOT-2 — we're gonna need thirty eight
13:12:23.7 HOT-1 — just tell me our brake situation
[Gulfstream Submission, ¶1.2
Source: Voice Recorder Transcript, p.12-52
- The PNF devoted his attention to completing the Left Hydraulic System (SYS) Failure-Loss of Pressure and Fluid checklist prior to landing and per step 14 selected Aux pump-ON, 16 seconds prior to Main Landing Gear (MLG) touchdown. With the landing imminent, the PNF discontinued his review of the checklist at this point, failing to note step 18 requiring the manual deployment of the speed brakes.
- The Digital Flight Data Recorder (DFDR) data did not indicate any system pressure rise in the Aux Hydraulic system and recorded that Aux System pressure remained below 200 PSI for the duration of the landing. The purpose for having the Aux pump selected ON was to provide continuous pressure to the brakes and steering after landing in the event of Left Hydraulic System failure.
- Five seconds prior to MLG touchdown, the DFDR records that no Aux Hydraulic system pressure was available and the Aux Hydraulic Fail message was displayed on the CAS System. Because the warning inhibit was selected ON per the normal checklist, there was no aural warning tone to inform the crew of the amber message indicating the loss of the Aux system. Touchdown airspeed was 137 KCAS, which was 12 knots faster than the scheduled Vref speed of 125 KCAS. The airplane landed long, using 2048 feet of runway before main gear touchdown, leaving 4453 feet remaining to stop the airplane. With no hydraulic fluid in the Left or Aux Hydraulic system, the ground spoilers could not auto deploy on landing because there was also no hydraulic pressure to the Ground Spoilers Control “pop-up” signal. The PF had throttles at idle and following MLG touchdown felt that it took a long time to get the nose down, which was a result of the ground spoilers not deploying. The DFDR indicated that approximately 8 seconds transpired from Main Landing Gear (MLG) touchdown to NLG touchdown. The PNF did not manually deploy the speed brakes per the emergency Left Hydraulic Fail checklist, which is a backup precaution in the event that the Ground Spoilers do not deploy.
- The PF commanded thrust reversers deployment, deploying only the right thrust reverser as the hydraulic failure prevented left thrust reverser deployment, and when pressing the brake pedals felt no braking action and reported initially reaching for the emergency brake. At this time, the Runway Awareness and Advisory System (RAAS) audio calls out “3000 remaining”. Six seconds later, RAAS calls out 2000 feet remaining and then 3 seconds after that callout the PF elected to initiate a balked landing, stowing the right thrust reverser and advancing the throttles to takeoff power, thinking that there was not enough distance remaining to stop. Three seconds later RAAS calls out 1000 remaining. With no engine acceleration and the airspeed stable at 101 KCAS, and approximately 1000 ft. remaining ( the DFDR/CVR recorded approximately 800 ft. remaining), the PNF, on his own initiative, pulled the throttles to idle.
- The PF seeing that they were going to depart the runway, commanded thrust reversers deployment, deploying only the right thrust reverser as the hydraulic failure continued to prevent left thrust reverser deployment, as the aircraft departed the end of the runway and directed his attention to avoiding an antennae array and two buildings. After clearing those obstacles, the aircraft traversed a shallow depression where the left main gear collapsed. The aircraft continued traveling approximately another 500 ft. before coming to a stop. The crew shut down the engines and exited the aircraft through the main entry door.
Source: NTSB Factual Report, pg. 1
3
Analysis
- As set out above, the amber L Hydraulic System Fail message directs the crew into the QRH emergency procedure checklist for “Left Hydraulic System Failure Loss of Pressure and Fluid”. Because the failure of the Left Hydraulic System occurred after the aircraft was configured to land, there was not sufficient time to complete all of the required steps in the emergency procedure checklist if the landing was to continue as planned. The PNF skipped the initial portion of the emergency procedure checklist and began reviewing the steps of the checklist at the point that matched the aircraft’s configuration for landing, i.e. “landing gear down and flaps 20”.
- By entering the emergency checklist at this step, the PNF did not read the specific caution at the beginning of the checklist: “To verify the availability of auxiliary system fluid, select the aux pump on for a minimum of 30 seconds and check for auxiliary system pressure. If pressure cannot be maintained, assume that the auxiliary system is not available and proceed to the Left System and Auxiliary Hydraulics System Loss of Fluid.”
- In accordance with the Before Landing Checklist and prior to entering the emergency checklist, the PNF had momentarily turned on the aux pump to charge the brake accumulator after the landing gear was extended. This may have led the PNF to a false confidence that the Aux system was operating even as he later would notice left hydraulic system warning messages.
- Had the crew noted and followed the caution at the very beginning of the procedure, they would have noticed that the pressure could not be maintained and would therefore be directed to a different emergency procedure checklist for “Left System and Auxiliary Hydraulics System Loss of Fluid.” This checklist directs the crew to select a runway that is at least 7000 feet long and 150 feet wide, plan a shallow approach, and to land within the first 1000 feet of the runway. It further states that “. . . for use of the Emergency Brake, increase pressure slowly to maintain 400 PSI. However it may be necessary to exceed this pressure in order to stop the airplane on the runway. The pilot should devote his attention to airplane control and brake application, while the copilot should monitor applied brake pressure, advising the pilot of corrections required to maintain optimum brake pressure.”
Source: Gulfstream Submission, ¶2.3
- A major contributor to the accident was the communications breakdown in CRM. The PNF who was responsible for running the emergency checklists, suggests that the landing be aborted, but did not verbalize to the pilot that his recommendation was based upon the time constraints of satisfactorily completing the emergency checklists, and was not forceful enough in communicating his opinion to the pilot. The PF meantime unilaterally decided to continue with the landing for a variety of reasons that were probably not verbalized to the PNF, but regardless did not justify landing without completing the checklists. There was no compelling safety of flight condition that required an immediate landing since the right hydraulic system was operational, as further evidenced by the crew having full flight controllability at all times, but the crew did not apparently discuss this fact either.
- The decision to land without determining beforehand the availability of braking capability defeated the CRM principal of maintaining situation awareness of the true nature of the problem, and the likely issues that may manifest themselves upon landing. The crew did not discuss alternatives and inoperative systems, including emergency braking procedures, and did not coordinate who was to activate the emergency brakes.
- Upon landing, the PF felt it took a long time to get nose gear touch down following MLG touchdown, apparently unaware that the aircraft’s ground spoilers would not deploy automatically with this hydraulic failure, and as a result of poor CRM, the PNF was not prepared to deploy the speed brakes manually.
- As the landing continued to develop, the PF made a unilateral decision to attempt a balked landing and moved the throttles forward. The PNF noted the airspeed was not accelerating fast enough with the end of the runway approaching and pulled the throttles to idle to avoid what he felt was a worst case scenario of continuing the takeoff and going off the end of the runway at an ever higher speed. This unilateral action by the PNF, while not representative of good CRM, probably saved the lives of the crew.
Source: Gulfstream Submission, ¶3
- Gulfstream’s post accident analysis shows that after the first 8 seconds of the balked landing command, there would be a brisk acceleration to rotation speed of 117 KCAS. Therefore the distance required to accelerate from the initiation of the balked landing to 117 KCAS is 2100 ft in 13 seconds. The normal rotation distance requires an additional 500 ft, resulting in a total distance of 2600ft for takeoff from the noted conditions. The FDR data indicated there was about 1777ft remaining available; therefore a successful balked landing could not be accomplished.
- There was no point during the landing that the crew attempted to use the emergency brake to stop the aircraft. The aircraft touched down with 4453 feet remaining of the 6501 feet runway length at 137 knots (132 knots ground speed). Approach speed for the weight and flaps 20 configuration was 125 knots. The pilot’s first attempt to brake was at 122 knots ground speed with 3000 feet remaining using normal pedal brakes, which were inoperative. For purposes of analysis, if the pilot had initiated braking through the use of the emergency brakes at 122 knots ground speed the analysis showed that it was not possible to stop the aircraft. Following the checklist procedure with the right thrust reverser deployed and using 400 psi with the emergency brake handle, the stopping distance from brake initiation at 122 knots ground speed to full stop is 4702 ft. This point of initial brake application analysis coincides at the same time the crew received oral RAAS 3000 feet remaining callout.
- In addition, had CRM been properly conducted, the crew would have followed the QRH instructions for “Left System and Auxiliary Hydraulics System Loss of Fluid”, the pilots would have selected the 8002 ft. runway at ATW, landed within the first 1000 feet of the runway threshold, and had over 7000 feet to execute a successful stop using 400 psi of emergency brake pressure.
Source: Gulfstream Submission, ¶4
- The Quick Reference Handbook procedure checklist for Left Hydraulic System Failure at the time of the accident had two separate procedures, one dealing with loss of Left system pressure and fluid, and the other dealing with loss of Left and Aux Hydraulic system. Both of those procedures had the identical caution with the statement: “To verify the availability of Auxiliary system fluid, select the Aux pump on for a minimum of 30 seconds and check for Auxiliary system pressure. If pressure cannot be maintained, assume that the Auxiliary system is not available and proceed to the Left System and Auxiliary Hydraulics System Loss of Fluid.”
- The reason for the caution on both checklists is that the synoptic indication of fluid in the Aux system is predicated on the piston position for fluid in the Left system reservoir and not the actual fluid in the Aux system. The only quantity enumerated is for the fluid in the Left system and not the Aux. If the Left system reservoir piston is positioned to empty, the Aux system will indicate empty, even if fluid is present. The only reliable check of fluid being present in the Aux system is the ability to maintain system pressure. That is why it is imperative for the crew to note the caution and complete the directed action.
- The change to the QRH in the case of experiencing a Left Hydraulic System failure now incorporates the assumption that upon the failure of the Left Hydraulic System, the Aux system is lost as well. The procedure plans for the worst case scenario of losing all Left and Aux fluid upon touchdown, directing the crew to prepare for landing without ground spoilers or normal braking. If the Aux System remains functional, landing and braking operations will be normal.
Source: Gulfstream Submission, ¶7
"Throughout my 20 year military carrier I was always taught that if you had a problem inside the final approach fix and your gear was down it was always better to land. We lost several aircraft because pilots delayed their landings. At Flight Safety in the GV and GIV training that I receive every 6 months I have never been given a scenario with a system malfunction were I would go around inside the final approach fix."
Source: PF's Statement to the NTSB
4
Cause
The National Transportation Safety Board determines that the probable cause of this accident was the captain's decision to attempt a go-around late in the landing roll with insufficient runway remaining. Contributing to the accident were (1) the pilots' poor crew coordination and lack of cockpit discipline; (2) fatigue, which likely impaired both pilots' performance; and (3) the failure of the Federal Aviation Administration (FAA) to require crew resource management (CRM) training and standard operating procedures (SOPs) for 14 CFR Part 135 operators.
Source: NTSB Factual Report, pg. 1j
- This accident could have been avoided with proper crew management of the hydraulic failure.
- The failure of the NWS swivel and loss of left and auxiliary hydraulic system established an emergency condition that was defined in the pilots’ QRH that when poorly managed by the flight crew caused the accident.
- While the crew was alerted to the left hydraulic system failure by the aircraft’s crew advisory system, the crew did not take the necessary time to complete the emergency checklists prior to landing. By failing to complete the required checklists, the crew unknowingly landed without normal ground spoiler and brake operation. Had the crew decided to go-around prior to landing, there would have been sufficient time to execute the required emergency checklists set out in the QRH in response to the CAS messages, As a result, the crew would have been advised on how to properly configured the aircraft, coordinate their cockpit duties, and execute a safe landing. The failure of the crew to perform this go-around before landing to brief themselves fully on the emergency and conduct proper Crew Resource Management preparations is the primary cause of this accident.
- Following the accident, Gulfstream determined that the emergency checklists for the relevant CAS messages displayed during the accident, while correct, required the crew to check whether or not the Auxiliary Hydraulic System was functional. A simpler emergency checklist which assumes a dual left hydraulic system failure and auxiliary system failure was published by Gulfstream in the Quick Reference Handbook for the G550 and will soon be published in other Gulfstream aircraft with similar dual system failure possibilities. The new emergency checklist and its assumption of auxiliary hydraulic system failure, reduces the number of checklists required and the new combined checklist quickly prepares the crew for landing without automatic deployment of ground spoilers, left Thrust Reverser, Nose Wheel Steering, and normal braking, preparing them to select a long runway, take a shallow approach, land within the first 1000 feet of the runway threshold, manually deploy speed brakes and prepare to deploy emergency brakes if normal braking is unavailable. If the hydraulic failure is not a dual failure disabling the auxiliary hydraulic system, the crew will be able to stop the aircraft using normal braking. Gulfstream believes this revision is a safety enhancement. Gulfstream does not believe that the emergency checklists as they existed at the time are a contributing factor to the accident.
- Putting aside the crew resource management issue addressed above, this accident could have been avoided by proper airmanship on the part of the experienced production/completion test pilot who was flying the aircraft. The PF has ultimate responsibility for determining whether a landing is safe to continue, and he should have aborted the landing on the first display of an amber caution message on the CAS. Having failed to do that, the PF was the crewmember responsible for brake application on touchdown and therefore the first crew member who was aware that the normal brakes were not working. The PF should have applied the emergency brakes as necessary to stop the aircraft on the runway, as he reports was his first intention. If he had done so, the likely result would have been that the aircraft would have been brought to a stop on the runway with little damage other than blown tires. Gulfstream believes the PF’s failure to apply emergency brakes is a contributing factor in this accident. Additionally, the PF’s decision to attempt to take off after he recognized the brake failure, and after the engines had been retarded to idle and the thrust reverser deployed, with less than 2000 feet of runway remaining, displayed very poor airmanship judgment. There was simply not enough runway left to get this aircraft airborne at this point in time. Gulfstream believes the PF’s decision to attempt to take off with this configuration and at this location on the runway was a contributing cause of the accident.
- Putting aside the crew resource management issue addressed above, a portion of which was the responsibility of the experienced production/completion test pilot who was not flying the aircraft; we commend the airmanship of the PNF for countermanding the PF’s decision to attempt to take off by unilaterally retarding the throttles and aborting the attempted take off. The PNFs proper action at this late stage in the accident sequence prevented even more serious damage to the aircraft and the possible loss of life of the three crew members aboard the aircraft.
Source: Gulfstream Submission, ¶8
References
(Source material)
Gulfstream G550 Quick Reference Handbook, GAC-AC-G550-OPS-0003, Revision 27, 24 July 2008
Gulfstream G550 Outfitting Check Flight Accident Gulfstream Party Submission, CEN11FA193, March 25th, 2013
NTSB Factual Report Aviation, CEN11FA193, N535GA, 02/14/2011, Appleton, WI.
NTSB Statement from the PF, CEN11FA193, N535GA, 02/14/2011, Appleton, WI.
NTSB Voice Recorder Transcript, CEN11FA193, N535GA, 02/14/2011, Appleton, WI.