Several years ago during a Gulfstream G550 pre-simulator session briefing the instructor said something that immediately caught my attention. “It takes a lot of precision to fly a non-precision instrument approach,” he stated matter-of-factly. I pondered for a moment on what he had just said and then jotted it down in my notes – word for word. Although I understood what he meant I had never heard anyone say it so eloquently. To this day I continue to refer to that statement and reflect on the implications of its meaning.
— Ivan Luciani

Updated:
2020-11-14

A Southern Airways DC-9
similar to Flight 932 (With permission,
Clipperartic - Slide via Collection)
Several years ago during a Gulfstream G550 pre-simulator session briefing the instructor said something that immediately caught my attention. “It takes a lot of precision to fly a non-precision instrument approach,” he stated matter-of-factly. I pondered for a moment on what he had just said and then jotted it down in my notes – word for word. Although I understood what he meant I had never heard anyone say it so eloquently. To this day I continue to refer to that statement and reflect on the implications of its meaning.
A non-precision instrument approach procedure lacks the electronic vertical guidance provided by a precision instrument approach procedure. That is, among other things, what makes a VOR, an NDB or a Localizer approach a non-precision procedure. Conversely, an ILS approach is classified as a precision procedure because – in addition to highly accurate lateral guidance – it provides highly accurate vertical guidance in the form of a glideslope signal. While the VOR, NDB or Localizer approaches offer less precision in terms of electronic guidance than the ILS, they each demand far more precision from the crew in their execution. That is exactly the message the G550 simulator instructor wanted to convey that day. Why is this important? Because anything less than total precision on the part of the crew in the execution of a non-precision instrument approach exponentially increases the chances of an approach and landing accident. Simply said, the margin for error is very small and its consequences much greater. This is a message worth understanding and remembering. Incidentally, according to the Flight Safety Foundation, 50% of all aviation accidents occur during the approach and landing phase of flight.
Years ago crews were taught the “dive and drive” technique as part of the execution of a non-precision instrument approach procedure. At the Final Approach Fix (FAF) the crew would initiate a rapid descent – the dive – to the procedure’s minimum descent altitude (MDA). Then, the crew would level off and maintain that altitude – the drive – until the runway environment was sighted and a normal descent and landing could be made. Failure to see the runway environment by the published missed approach point would require the crew to immediately initiate the published missed approach procedure. The purpose and rationale for the “dive and drive” technique was to descend below the ceiling to the MDA in order to help the crew sight the runway early enough to allow for a final descent and normal landing.
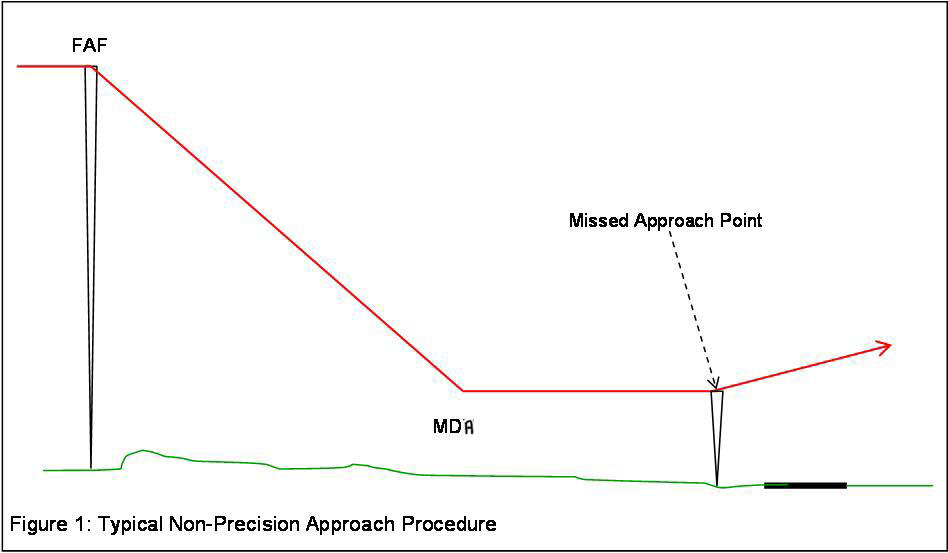
“dive and drive” technique,
(Skybrary)
Once visual with the runway environment, and the landing assured, the crew would then set flaps to landing. This last minute aircraft configuration change would require pitch trim and engine thrust adjustments as the aircraft was slowed down to its final approach speed. Even for highly disciplined and experienced crews the slightest deviation from total precision in the execution of a non-precision approach, even momentarily, could potentially result in a Controlled Flight Into Terrain (CFIT) accident, a loss of control (LOC) accident or a runway excursion.
In the case of Southern Airways 932, the crew had to deal with poor weather conditions while executing a non-precision instrument approach procedure at night over hilly terrain and into an unfamiliar airport to a relatively short and wet runway. None of these factors, taken individually or collectively, necessarily make non-precision approaches unsafe…provided the crew’s execution of such approaches is precise.
Flight 932 has been classified as a CFIT accident which, by definition, refers to the collision with the ground, an obstacle or a body of water of a fully functioning aircraft with the crew being unaware of the impending impact. In other words, the crew did not realize they were about to crash their airworthy aircraft or realized it too late to prevent it. At the time of this particular accident, Flight 932 was the 14th worst accident in the United States of America.

1
Accident report
- Date: 14 November 1970
- Time: 19:36 EST
- Type: DC-9
- Operator: Southern Airways
- Registration: N97S
- Fatalities: 4 of 4 crew, 71 of 71 passengers
- Aircraft Fate: Destroyed
- Phase: Approach and landing
- Airport: (Departure) Kinston-Stallings Field (KISO), NC, USA
- Airport: (Destination) Huntington-Tri-State Airport, WV (KHTS), USA
2
Narrative
Synopsis
Southern Airways, Inc., a DC-9, N97S, operating as charter Flight 932, crashed during a landing attempt at the Tri-State Airport, Huntington, West Virginia, at approximately 1936 E.S.T., on November 14, 1970. All 75 occupants, including 71 passengers and four crewmembers, were fatally injured. The aircraft was destroyed.
The flight, chartered to transport the Marshall University football team and boosters from Kinston, North Carolina, to Huntington, West Virginia, was attempting a non-precision instrument landing approach to runway 11 at the time of the accident. The crash occurred following impact with trees on a hill approximately 1 mile west of the runway threshold. The elevation of the broken trees at the initial impact site was approximately 922 feet M.S.L. The Minimum Descent Altitude, below which a descent is not authorized until the runway environment is in sight, for this instrument approach was 1,240 feet M.S.L.
The weather at the time of the accident was: 300 feet scattered, estimated 500 feet variable broken, 1,100 feet overcast, visibility five miles, light rain, fog, smoke, wind 360° at 4 knots, altimeter setting 29.67, ceiling ragged and variable 400 to 600 feet.
Source: NTSB AAR-72-11, Excerpts
The flight:
Southern Airways Charter Flight 932 (SOU 932) was scheduled as a ferry flight from Atlanta, Georgia, to Kinston, North Carolina, to return members of the Marshall University football team, the coaching staff, and other passengers to Huntington, West Virginia, from Kinston.
Source: NTSB AAR-72-11, Excerpts
1970 Marshall Thundering Herd football team, (with permission: https://www.marshall.edu/special-collections/memorial/)
The flight departed Atlanta at 1548 and arrived at Kinston at 1642. The aircraft was refueled, but no maintenance was requested or performed. Seventy passengers boarded the aircraft and the flight taxied from the ramp at 1828 with a total of 75 persons aboard.
The captain filed an Instrument Flight Rules (IFR) flight plan to Huntington, via direct Raleigh-Durham, North Carolina, direct Pulaski, Virginia, direct Huntington, at Flight Level 260 (FL 260 ). The true airspeed was 473 knots and the estimated time en route was 52 minutes. The flight departed Kinston at 1838 and proceeded in accordance with the flight plan.
Source: NTSB AAR-72-11, Excerpts
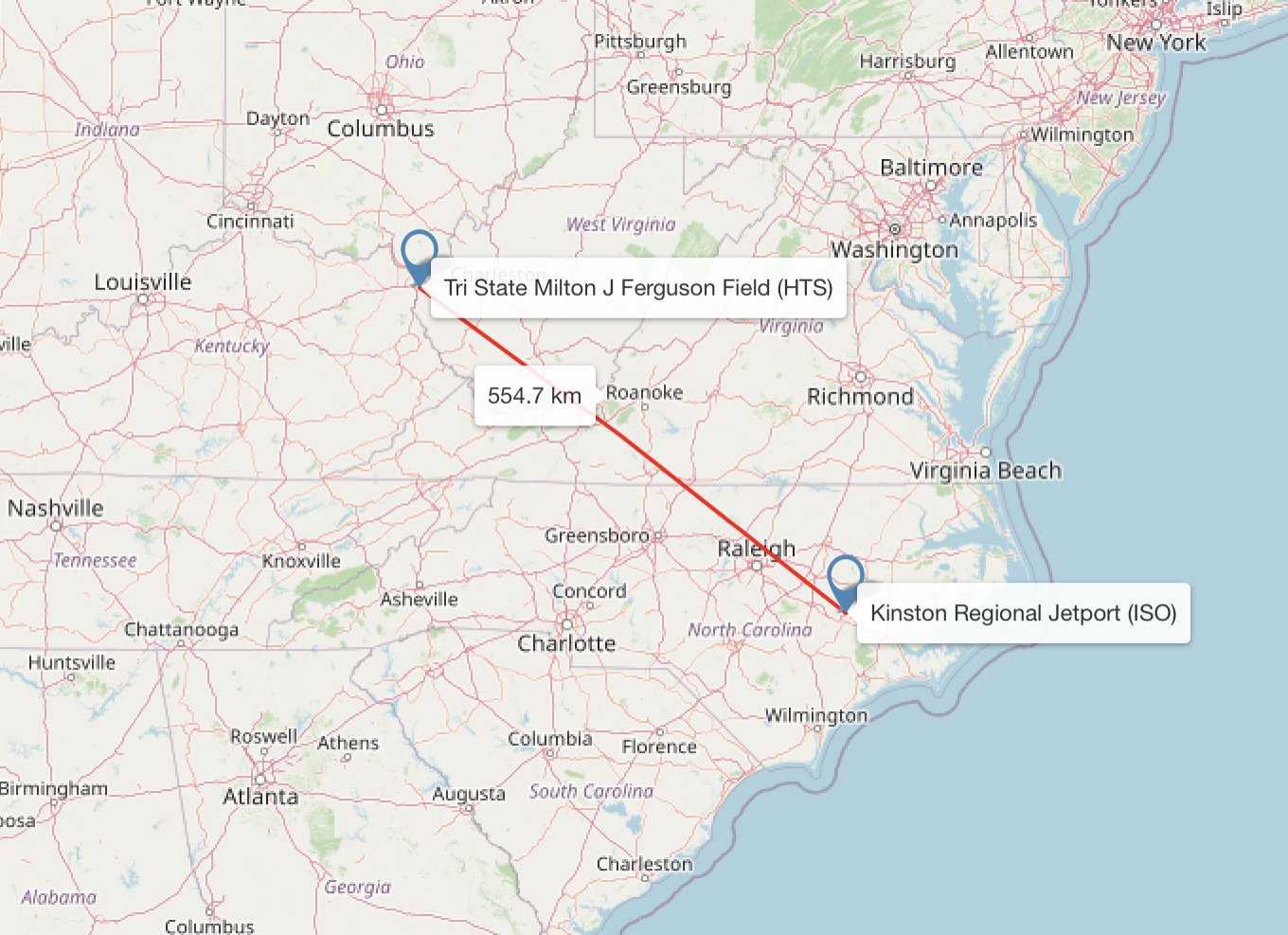
(free map tools)
SOU 932 established contact with Huntington Approach Control by advising “. . . we’re descending to five thousand.” The controller cleared them for a localizer approach to Runway 11 and added, “…the surface winds are favoring runway twenty-nine, three five zero degrees at six, altimeter two niner six seven…” the crew acknowledged this information and then the controller advised, “…the Huntington weather three hundred scattered, measured ceiling five hundred, variable broken, one thousand one hundred overcast, visibility five, light rain, fog, smoke, ceiling ragged variable four to six hundred.”
At approximately 1933, the captain said that he could fly at 130 knots, and the first officer responded that he was checking the time, and the approach should take 2 minutes, at 1934, the crew reported passing the outer marker inbound, and they were cleared to land. The wind was then reported as 360° at 7 knots. Following a discussion of the approach lighting during which the crew requested “step three,” the tower controller stated, “Roger, that’s where they are, with the rabbit (sequence flasher). Advise when you want them cut.” At approximately 1936, tower personnel observed a red glow west of the airport. When no response to subsequent radio calls was received, the tower controller initiated the emergency procedures.
The last flight to operate into Huntington prior to SOU 932 landed on Runway 11 at 1848 and departed at 1907. The captain of that flight stated that the weather was essentially as reported to him, 300 feet scattered, 500 feet variable broken. They broke out of the clouds at minimums, west of the refinery (located approximately 2 miles west of the airport). The forward visibility was good, and the runway was in sight from this point until they landed, although they did encounter some widely scattered clouds.
The aircraft initially struck trees in a hill 5,543 feet west of the runway threshold, and cut a swatch 95 feet wide and 279 feet long through the trees in a bearing of 110°, 122 feet right of the runway centerline extended. The main wreckage site was located 4,219 feet from the threshold of Runway 11, and approximately 225 feet south of the middle marker. The ground elevation at the initial tree impact was 860 feet M.S.L., and the elevation at the break in the tree at this location was 916 feet 2 inches M.S.L. This was a non-survivable accident.
Source: NTSB AAR-72-11, Excerpts
3
Analysis
The aircraft center of gravity was within allowable limits. Based on the aircraft performance capability, there was sufficient runway available for N92S to have landed under the conditions existing at Huntington at the time of the accident.
The crew was properly certificated and qualified for the flight. The aircraft had been maintained in accordance with existing company procedures and the Federal Aviation Regulations. The investigation disclosed no malfunctions or failure in the aircraft structure, primary flight controls, or powerplants.
The Board reviewed the charter arrangements, operations specifications, and regulations governing the dispatch and conduct of this flight. Although the flight was conducted in accordance with the prescribed procedures, there is one area which is of concern to the Board.
An equivalent level of safety for “off route” operations, of the type involved in this accidents, is theoretically achieved by the increased landing minima applicable to such operations. However, the crew requirements for “off route” airport qualifications do not require the same degree of qualification as that required for scheduled operations. The reason for this is that it would not be practical to require an actual entry into every possible “off route” airport, nor would it be practical to have on hand the approved pictorial display for every possible “off route” airport. There is no evidence in this case to indicate that the crew had not sufficiently familiarized itself with the Huntington airport, surrounding terrain, and the approach and landing procedures. At the same time, there is no way to assure that the crew had actual knowledge of the foregoing prior to departure.
The flight path and profile show that the aircraft descended through the MDA approximately 2 miles from the end of the runway and that such descent was not corrected in time to avoid impact with the trees. Conversation between the captain and first officer during the 10-second period preceding the MDA passage indicates that they were beginning to see the lights on the ground, or at least the glow of the lights. It is possible that the sighting of these lights, in combination with the knowledge that they were approaching the bottom of the lowest cloud layer, could have induced the Captain to continue descent below MDA in order to see the runway environment at the earliest moment. The descent, in fact, did continue through this period, and ground witness observed the aircraft clear of clouds in this area.
It is also possible that the conduct of the approach could have been affected by a visual illusion produced by the difference in the elevation of the refinery and the airport. Approximately, 2 miles from the runway, the flight was approaching the bright lights surrounding the refinery and, as noted above, the crew was discussing at least the glow, and probably fleeting glimpses, of ground lights through the broken clouds. As the descent continued, the opportunity for ground reference through scattered clouds would have increased. Below approximately 1,100 M.S.L., the only restriction to visibility should have been the fog, smoke, and light rain.
If the approach lights or sequence flasher lights were sighted while the refinery lights were still in the field of vision, with no appreciable lights between, the pilots would have mentally visualized both light sources at the same elevation as the nearer lights. Therefore, the height above both lights would appear to be about 700 feet, whereas the actual height above the approach lights would have been only 400 feet, due to the 300-foot difference in elevation between the refinery and the approach lights. After the aircraft passed the refinery, the preconceived image would have been retained and the visual cues would have told the crew that they were approximately 300 feet higher than desired.
The remaining evidence, however, strongly suggest that the crew never obtained visual contact with the approach lights or with any part of the runway environment. The visual illusions discussed above, for example, would have prompted an increase in the rate of descent, which significantly is not reflected on the flight data recorder. Even more important, there were no comments on the cockpit voice recorder pertaining to ground lights other than those mentioned as the aircraft passed over the refinery. If any lights associated with the runway environment had been sighted, it can be presumed that some mention of the sighting would have been made. Certainly such a presumption is far more likely than the explanation that the runway environment was sighted, but that such sighting was either sufficiently obvious to negate the need for a callout or was indicated and acknowledged by nonverbal signals.
The recorded conversation also indicates that the crew was not aware that the aircraft had descended below MDA. The first officer’s comment at 1935:06 “We are two hundred above” is most logically construed as a reference to MDA. The following comment by the charter coordinator (riding in the jump seat) “Bet’ll be a missed approach” can be taken to mean that the flight was approaching MDA, yet the runway environment was still not in sight. The next statement on the recorder (“Four Hundred”) most probably means that the aircraft had reached MDA, which is 400 feet above the airport elevation. Such interpretation is consistent with the following remark of the captain (“that the approach?”), which indicates that he was asking, perhaps rhetorically, whether they had reached the farthest point to which the flight could legally descend. The first officer responded, “Yeah,” which again implies that the MDA had been reached and the runway environment was not in sight. The available evidence also indicates that a level off or missed-approach was then initiated. The swath cut through the trees, ground witnesses statements, and the flight recorder altitude trace all show that the descent was stopped, power was added, and a gradual climb was commenced. Furthermore, the first officer called out airspeed in terms of a number (“Hundred and twenty-six”) instead of a reference speed (“bug plus- - -“), which is indicative of a go-around rather than a continuing approach.
In view of the foregoing, the Board concludes that the crew never sighted the runway environment and was not aware that the flight had descended through actual MDA.
Source: NTSB AAR-72-11, Excerpts
4
Cause
The National Transportation Safety Board determines that the probable cause of this accident was the descent below Minimum Descent Altitude during a non-precision approach under adverse operating conditions, without visual contact with the runway environment. The Board has been unable to determine the reason for this descent, although the two most likely explanations are (a) improper use of cockpit instrumentation data, or (b) an altimetry system error.
Source: NTSB AAR-72-11, Excerpts
5
Ivan's take
A lot of things have changed since this tragic event. Lessons from Flight 932, as well as from many other accidents, eventually led to the development and adoption of Crew Resource Management (CRM) as a core operating philosophy, the establishment of the Sterile Cockpit concept, the implementation of the stabilized approach criteria, the substitution of “dive and drive” in favor of the Constant Descent Final Approach (CDFA) procedure, and many others. From a technological point of view we have seen the development and implementation of Terrain Awareness and Warning Systems (TAWS), Synthetic Vision Systems (SVS), Enhanced Flight Vision Systems (EFVS), and others. These, and other procedural and technological improvements, have had a tangible effect on today’s impressive safety record. That is certainly great news but let us never forget – or take for granted – the high price that has been paid for it.
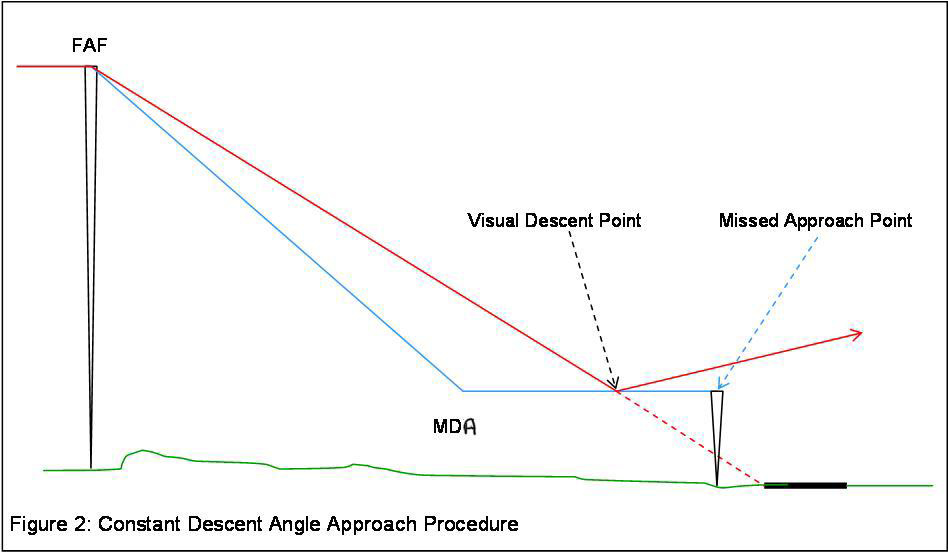
Constant Descent Final Approach (red), (Skybrary
Yes, a lot has certainly changed over the past 50 years and that includes how we execute non-precision instrument approaches. However, many of the lessons learned remain relevant today. Case in point, I am currently flying a Gulfstream G650, one of the most advanced business jets and Gulfstream’s current flagship. A G650 is equipped with the latest and greatest technological systems but that does not preclude the need for the crew to fly a non-precision approach with exact precision. On a recent trip to an unfamiliar airport we had to execute an RNAV approach, a non-precision instrument approach, to LNAV minimums. This GPS-based procedure provided us precise lateral navigation to the runway but not vertical guidance. Just prior to passing the FAF, and already fully configured for landing, Flight Path Angle (FPA) was manually engaged as a vertical mode. The use of FPA allowed us to accurately descend in a stabilized manner at the published path angle to the Derived Decision Altitude (DDA). Had the runway environment not been in sight as we reached DDA (MDA + 50 feet) we would have had to execute a go around. Conversely, and as it actually happened, with the runway environment in sight as we descended through DDA we were already in a position from which a stabilized visual descent could be continued and a normal landing made.
Although there is no longer a need to “dive and drive” and to make last minute configuration changes the lesson from that G550 simulator instructor was still at the forefront of my mind during that RNAV approach. Technology and improved procedures have made the execution of non-precision instrument approaches much easier and a lot safer but the need for exact precision on the part of the crew remains just as critical. In fact, I would argue that with today’s highly automated flight decks the need for the crew to remain even more vigilant goes hand in hand with the need for exact precision in execution. Furthermore, because we carry out fewer non-precision approaches these days there is another factor that must be considered: reduced proficiency level in the execution of these approaches.
To conclude, “It takes a lot of precision to fly a non-precision instrument approach.” That is a lesson still worth remembering, sharing…and adhering to.
Lastly, and as a tribute to the people who perished in Flight 932, as well as to their families and friends, I would like to end this article by saying . . . We are Marshall!
References
(Source material)
Flight Safety Foundation - Aviation Safety Network
Flight Safety Foundation - Skybrary - CDFA
Flight Safety Foundation - Skybrary - Approach and Landing Accidents
NTSB Aircraft Accident Brief, AAR-72-11, Southern Airways, Inc. Douglas DC-9 N97, Tri-State Airport, Huntington, West Virginia, November 14, 1970