At what point during the takeoff is an abort no longer an option unless the airplane is unflyable? V1? Yeah, that's as it should be. Now, what if you have already pulled the nose back to rotate and the nose does come up? Would you consider an abort then?
— James Albright

Updated:
2017-09-15

US Airways 1702, (Facebook / Dennis Fee)
A ridiculous question? Watch this video, keeping an eye on the upper left as it begins: US Airways 1702.
We practice takeoff aborts ad nauseam during training and we have drilled into our heads that after V1 the takeoff will not be aborted unless the airplane will not fly. Every now and then, believe it or not, we have someone abort a takeoff after the takeoff. This particular captain's union came to his defense, saying he had never been trained for this exact situation. I could spell out the lesson here, but it is obvious, isn't it?
I quote the accident report liberally and add my own comments. If you are a captain from an airline with the philosophy that abort authority should never be divided, you will probably object to these comments. They are, of course, my opinions. I speculate a lot on this page, doing what many will say is second-guessing the crew. I am indeed, but that is my purpose here: to show the pitfalls of this abort authority philosophy. More about this: Abort Authority.

1
Accident report
- Date: 13 March 2014
- Time: 18:30
- Type: Airbus A320-214
- Operator: US Airways
- Registration: N113UW
- Fatalities: 0 of 5 crew, 0 of 149 passengers
- Aircraft fate: Substantially damaged
- Phase: Takeoff
- Airport (departure): Philadelphia International Airport (KPHL), Pennsylvania, U.S.A.
- Airport (arrival): Fort Lauderdale International Airport (KFLL), Florida, U.S.A.
2
Narrative
Here is the "Reader's Digest" version of what happened. The first officer failed to properly program the FMS, both pilots failed to notice they didn't have V-speeds, and both pilots ignored several warnings that were worthy of a low speed abort. The captain elected to ignore early anomalies at 86 knots, "because procedurally they were at a high speed." But at 167 knots (10 knots above V1) and after he had already begun the takeoff rotation, the captain changed his mind.
- The first officer initialized the flight management computer (FMC) with the air traffic control (ATC)-provided flight plan and manually entered the departure runway into the FMC. Both pilots stated during postaccident interviews that they verified the ATC routing loaded into the FMC while still at the gate before pushback; however, neither pilot realized that the departure runway loaded into the FMC was runway 27R instead of the assigned runway 27L.
- The weather reported at 1754 was clear skies and 10 statute miles visibility, temperature 0°C, dewpoint - 21°C, and winds from 290° at 18 knots with gusts to 28 knots (peak winds at 1713 were recorded from 300° and 33 knots). Automatic terminal information service information "Yankee" called for runway 27L as the departure runway.
- At 1808:20, flight 1702 contacted ground control for taxi instructions; the ATC ground controller advised that the departure runway was 27L and provided taxi instructions to runway 27L.
- At 1822:35, flight 1702 was cleared to line up and wait on runway 27L. The first officer accomplished the remainder of the Taxi checklist. As the captain taxied onto runway 27L, he noticed that runway 27R had been inserted into the FMC instead of runway 27L and requested that the first officer change the runway in the FMC, which was completed at 1823:10.
Source: NTSB Report DCA14MA081, p. 4
Both pilots acknowledged that changing the runway in the FMC was fairly routine, but asking for this after being cleared onto the runway puts time pressure on the person making the change, and that makes the operation prone to error.
- At 1823:26, flight 1702 was given a heading of 230 degrees on departure and a clearance for takeoff. Flight data recorder (FDR) data indicate that the airplane had a ground speed of 0 knots indicated airspeed (KIAS) for about 11 seconds before accelerating for takeoff. At 1823:34, the throttle levers initially advanced to the MAX CLIMB level and the captain's longitudinal control was moved to the airplane nose down (AND) direction at 1823:41. The throttles were advanced further to the FLEX detent by 1823:43, with the airplane moving about 46 KIAS. According to crew interviews and cockpit voice recorder (CVR) data, when the captain set the thrust levers in the FLEX detent at 1823:45, the crew received an electronic centralized aircraft monitoring (ECAM) message and chime at 1823:47 indicating that the thrust was not set. In response, the first officer stated "engine thrust levers not set." FDR data indicate the thrust levers were briefly reduced to the climb detent then returned to the FLEX detent about 1 second later. The captain responded "they're set" 3 seconds later.
Source: NTSB Report DCA14MA081, p. 4
I learned early on in automated cockpits that if you have a "what's it doing now?" moment, chances are it is doing exactly as programmed and now the airplane will be operating outside your intentions. When you are flying this can be problematic and you just have to deal with it. During the takeoff roll you will need to be at your highest level of performance to deal with it. But before the aircraft picks up enough speed to make stopping risky, say 80 knots, you have the perfect opportunity to straighten things out. Most pilots know this intuitively. When the captain bypasses this option, it places a great deal on the first officer to either speak up or shut up.
- According to FDR and CVR data, the first officer did not make a required callout as the airplane's speed reached 80 KIAS. According to flight crew interviews, the captain and first officer noticed that there were no V-speeds indicated on their primary flight displays (PFDs), and FDR and CVR data show that as the airplane accelerated through 86 KIAS as an aural RETARD alert sounded in the cockpit. According to the CVR, at 1823:56, the captain asked the first officer "what did you do, you didn't load. We lost everything." At 1824:03, as the airplane continued to accelerate through 143 KIAS, the captain stated "we'll get that straight when we get airborne" and continued the takeoff roll.
Source: NTSB Report DCA14MA081, p. 4
Interviews with US Airways instructor pilots confirmed that SOP would be to discontinue to the takeoff if there were no V-speeds. Simulator tests confirmed they should have got a "Check Take Off Data" message in the scratch pad of the FMC. The captain later said that he thought 86 knots was in the high speed range and aborting because he didn't have V-speeds was too risky. I suppose. But I think he knew that was the wrong decision, as evidenced by his comment a few seconds later. The fact his reaction then was to blame the first officer shows his cockpit was his, and not theirs.
- The airplane continued to accelerate over the next several seconds, reaching 152 KIAS at 1824:08. At 1824:09, the first officer stated "wh*. I'm sorry", the captain's longitudinal control was brought into the airplane nose up (ANU) direction, and the pitch of the airplane began to increase as the longitudinal control was brought up to 6.9 degrees ANU over the next second as the airplane began initial rotation for takeoff. The airspeed at this point was 164 KIAS, and the nose gear weight on wheels discrete changed to "air" by 1824:10.
Source: NTSB Report DCA14MA081, p. 4
Having the "Retard!" aural alert yelling at you at this point can't be helpful. Interviews with several US Airways pilots of the same Airbus type revealed none had this experience. What does the "Retard!" alert sound like? Here is a short clip: Airbus A320 Retard.
What follows appears to be purely pilot induced oscillations, something you don't often see in this phase of flight, but the solution is the same in all cases: freeze the stick where it needs to be and let everything else settle down.
- Over the next 4 seconds, with the nose gear discrete reading "air" and the main landing gear discrete reading "ground" the captain's longitudinal control was pushed into the airplane nose down (AND) direction, and then pulled back in the ANU direction two times, reaching the maximum of 16 degrees in the ANU direction, and a minimum of 16 degrees AND during the cyclic input. The pitch of the airplane, and vertical acceleration followed the variations in longitudinal inputs. As the vertical acceleration decreased in response to the nose down input, the flight crew reduced the thrust levers, and the captain's longitudinal control was pulled again in the ANU direction. The vertical acceleration reached a minimum of 0.121 G as the control was pulled to 16 degrees ANU, the maximum operational value, and the engine throttle lever angles were reduced to idle thrust where they remained for the rest of the recording.
- By 1824:14, the nose gear weight on wheels discrete parameter changed back to "ground." During the previous 4 seconds, when the nose parameter recorded "air," the main landing gear (both left and right) weight on wheels parameter had recorded "ground," and the maximum radio altitude recorded was 6 feet above ground level (agl), which occurred for only 1 second.
- Once the pitch reduced to -0.4 degree, the vertical acceleration rapidly increased to 3.7 G, consistent with the gear impacting the runway surface. The pitch parameter was not valid for the rest of the FDR recording. As the vertical acceleration reached its maximum value, the captain's longitudinal input reached a maximum of 16 degrees ANU.
- The captain's longitudinal control cycled in the nose up and nose down directions over the next 2 seconds. During this variation, the vertical acceleration dropped to 0.47 G, then increased to 1.2 G. As the longitudinal stick was pulled back to over 16 degrees ANU and held at the maximum value, the main landing gear weight on wheel parameters changed to "air" for the next 2 seconds, and the radio altitude began to increase to about 15 ft agl.
- As the airplane reached 15 ft agl, the longitudinal control moved back to the AND position, and pitch of the airplane again reduced and the airplane began to descend back to the runway surface. The stick was moved again in the ANU direction as the airplane began to descend and, correspondingly, the airplane pitch increased again. Surveillance video obtained from the Philadelphia Airport captured the final impact with the runway. The video shows the airplane impacted the runway first with the tail, then main landing gear, and the airplane then rotated in the AND direction, resulting in the nose gear impacting the runway and subsequently collapsing.
- At 1824:48, the flight crew advised the tower that they aborted the takeoff as the airplane came to rest on the left side of runway 27L. At 1829:14, the flight crew advised the PHL tower that they were evacuating the airplane. The flight attendants stated all slides deployed normally, except door 2R, which was not deployed due to smoke on the right side of the airplane, and 2L, which did not reach the ground due to the nose gear collapse.
Source: NTSB Report DCA14MA081, p. 4
The video: US Airways 1702.
3
Analysis
Both pilots were highly experienced with the airline and in type, but both appeared to be failed pilots in terms of adherence to SOPs and the precepts of effective Crew Resource Management (CRM). The first officer made a common mistake when programming the FMC with the takeoff runway. The captain asked her to correct that after they cleared onto the runway and she missed one step, which meant they wouldn't have V-speeds and the system wouldn't understand why the thrust levers were set to a reduced setting, and not to takeoff thrust. The first officer made only minimal callouts as the problems started to cascade and eventually stopped communicating. The captain made a series of bad decisions followed by very erratic pitch inputs.
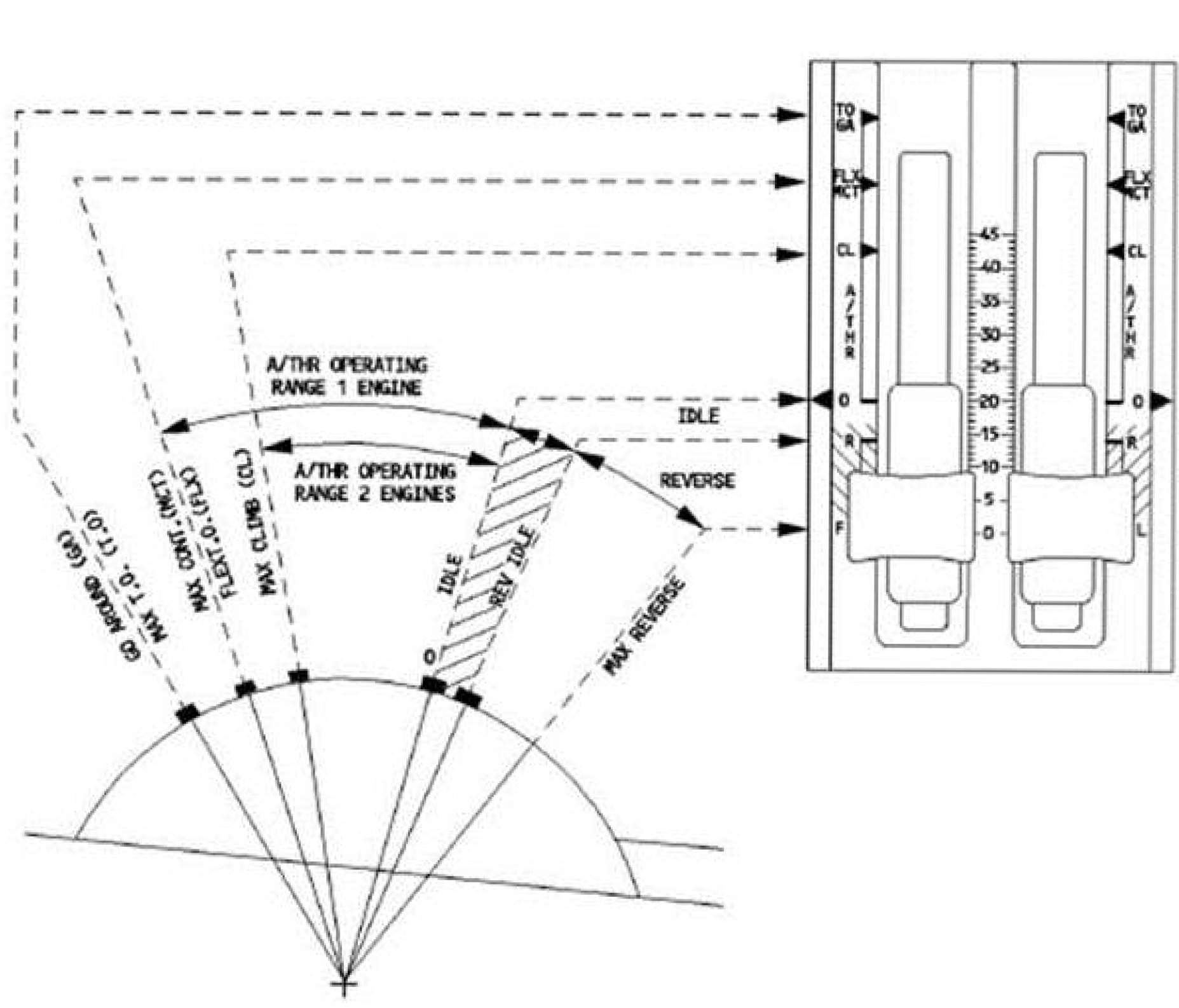
A320 thrust lever positions, NTSB Report DCA14MA081, figure 1
- Before pushback from the gate, the first officer, who was the pilot monitoring, initialized the flight management computer (FMC) and mistakenly entered the incorrect departure runway (27R instead of the assigned 27L). As the captain taxied onto runway 27L for departure, he noticed that the wrong runway was entered in the FMC. The captain asked the first officer to correct the runway entry in the FMC, which she completed about 27 seconds before the beginning of the takeoff roll; however, she did not enter the FLEX temperature (a reduced takeoff thrust setting) for the newly entered runway or upload the related V-speeds. As a result, the FMC's ability to execute a FLEX power takeoff was invalidated, and V-speeds did not appear on the primary flight display (PFD) or the multipurpose control display unit during the takeoff roll.
Source: NTSB Report DCA14MA081, p. 1
Subsequent simulator tests confirm they should have received a "CHECK TAKE OFF DATA" message in their FMS but the first officer does not recall seeing this.
- According to the captain, once the airplane was cleared for takeoff on runway 27L, he set FLEX thrust with the thrust levers, and he felt that the performance and acceleration of the airplane on the takeoff roll was normal. About 2 seconds later, as the airplane reached about 56 knots indicated airspeed (KIAS), cockpit voice recorder (CVR) data indicate that the flight crew received a single level two caution chime and an electronic centralized aircraft monitoring (ECAM) message indicating that the thrust was not set correctly. The first officer called "engine thrust levers not set." According to the operator's pilot handbook, in response to an "engine thrust levers not set" ECAM message, the thrust levers should be moved to the takeoff/go around (TO/GA) detent.
- However, the captain responded by saying "they're set" and moving the thrust levers from the FLEX position to the CL (climb) detent then back to the FLEX position. As the airplane continued to accelerate, the first officer did not make a callout at 80 KIAS, as required by the operator's standard operating procedures (SOPs).
Source: NTSB Report DCA14MA081, p. 1
- According to Airbus, the "ENG THR LEVERS NOT SET" ECAM message and associated chime is triggered on the A320 within 3 seconds of the thrust levers being placed above the climb detent. The FLEX takeoff mode was armed only if the flight crew entered a FLEX TO TEMP on the MCDU that was above the outside air temperature, or OAT. The US Airways A320 ECAM Supplemental Manual, page 506, also states the following:
If the flex mode is not armed, and the flight crew sets the thrust levers below or at the MCT/FLX position:
THR LEVERS . . . . . . . . . . TO/GA
Source: NTSB Report DCA14MA081, p. 12
This seems to be an easy fix that is right in the US Airway manual, but it must have been obscure because not a single US Airways pilot who was asked knew about it.
- According the FDR data and accident crew interviews, the thrust levers were never placed in the TO/GA position on the accident flight. According to the Airbus A320 FCOM, Abnormal and Emergency Procedures – Powerplant, page 251/256, when thrust levers are set to FLEX without a FLEX temperature and the flight crew does not set the thrust levers to the TO/GA position, the FADEC will automatically select TO/GA thrust after 8 seconds. When asked why he did not push the thrust to TO/GA after he received the "ENG THR LEVERS NOT SET" ECAM message and chime, the captain reported that it was "no harm" and left the thrust in FLEX. He also said he did not reject the takeoff at that point because he had already briefed a FLEX takeoff and he did not know the speeds and assumed temperature had dropped out.
Source: NTSB Report DCA14MA081, p. 12
The "No Harm" statement appears to be indicative of a pilot who thinks he or she knows better how to fly the airplane than the manufacturer.
"Retard"
- As the airplane reached 86 KIAS, the automated RETARD aural alert sounded and continued until the end of the CVR recording. According to Airbus, the RETARD alert is designed to occur at 20 ft radio altitude on landing and advise the pilot to reduce the thrust levers to idle. The captain later reported that he had never heard an aural RETARD alert on takeoff, only knew of it on landing, and did not know what it was telling him. He further said that when the RETARD aural alert sounded, he did not plan to reject the takeoff because they were in a high-speed regime, they had no red warning lights, and there was nothing to suggest that the takeoff should be rejected.
Source: NTSB Report DCA14MA081, p. 1
Had the captain selected the TO/GA thrust lever position the RETARD aural alert would not have happened. But very few Airbus pilots knew about this anomaly.
- The first officer later reported that there were no V-speeds depicted on the PFD and, thus, she could not call V1 or VR during the takeoff. She was not aware of any guidance or procedure that recommended rejecting or continuing a takeoff when there were no V-speeds displayed. She further said she "assumed [the captain] wouldn't continue to takeoff if he did not know the V-speeds."
Source: NTSB Report DCA14MA081, p. 1
It appears the first officer had frozen up with indecision, given the situation was outside of her experience. Asked about the situation, most US Airways instructors said the situation called for an abort. But the first officer wasn't authorized to call the abort. In this situation, since she couldn't simply say "Abort!" she had to formulate her message, such as "No V-speeds, maybe we should try it again." Faced with this task, she may have simply locked up. Her assumption that the captain would abort is a grave failing of CRM on her part and CRM culture on the part of the airline. But she wasn't alone in failed CRM:
- The captain stated that he had recalled the V-speeds as previously briefed from the Taxi checklist, which happened to be the same V-speeds for runway 27L. The captain continued the takeoff roll despite the lack of displayed V-speeds, no callouts from the first officer, and the continued and repeated RETARD aural alert.
Source: NTSB Report DCA14MA081, p. 12
- . . . according to an Airbus in-service information bulletin that was first made available to all operators in August 2008 and again in December 2013, a RETARD aural alert may be generated during a takeoff roll due to an FWC computation that did not match the flight phase. A divergence between an FWC computation and flight phase may be due to an abnormal thrust setting (that is, no engines recognized at takeoff power by the FWC). In the accident scenario, the abnormal thrust setting is due to a missing FLEX temperature and TLA remaining in the FLEX detent.
- According to Airbus, the RETARD aural alert on takeoff could be silenced by adhering to the ECAM procedure and setting the instructed thrust (TO/GA in this case). According to interviews conducted for the investigation, none of the US Airways A320 line pilots or A320 check airmen had ever heard that a RETARD alert could occur on takeoff before the flight 1702 accident. Airbus and US Airways training and manuals contain no guidance to pilots indicating how to respond to a RETARD alert on takeoff.
Source: NTSB Report DCA14MA081, p. 18
Rotation / Abort
- FDR data show that the airplane rotated at 164 KIAS. However, in a postaccident interview, the captain stated that he "had the perception the aircraft was unsafe to fly" and that he decided "the safest action was not to continue," so he commenced a rejected takeoff. FDR data indicate that the captain reduced the engines to idle and made an airplane-nose-down input as the airplane reached 167 KIAS (well above the V1 speed of 157 KIAS) and achieved a 6.7 degree nose-high attitude. The airplane's pitch decreased until the nosegear contacted the runway.
- However, the airplane then bounced back into the air and achieved a radio altitude of about 15 ft. Video from airport security cameras show the airplane fully above the runway surface after the bounce. The tail of the airplane then struck the runway surface, followed by the main landing gear then the nose landing gear, resulting in its fracture. The airplane slid to its final resting position on the left side of runway 27L.
- The operator's SOPs address the conditions under which a rejected takeoff should be performed within both low-speed (below 80 KIAS) and high-speed (between 80 KIAS and V1) regimes but provide no guidance for rejecting a takeoff after V1 and rotation. Simulator testing performed after the accident demonstrated that increasing the thrust levers to the TO/GA detent, as required by SOPs upon the activation of the "thrust not set" ECAM message, would have silenced the RETARD aural alert. At the time of the accident, neither the operator's training program nor manuals provided to flight crews specifically addressed what to do in the event the RETARD alert occurred during takeoff; although, 9 months before the accident, US Airways published a safety article regarding the conditions under which the alert would activate during takeoff. The operator's postaccident actions include a policy change (published via bulletin) to its pilot handbook specifying that moving the thrust levers to the TO/GA detent will cancel the RETARD aural alert.
Source: NTSB Report DCA14MA081, p. 2
I first started using the two-stage abort criteria in 1986, as taught by United Airlines to our Air Force Boeing 747 crews. We used 100 knots and V1. The industry standard seems to have become 80 knots and V1. I wonder if reclassifying the high speed abort range to start at 100 knots instead of 80 knots might have changed the captain's decision.
- Although simulator testing indicated that the airplane was capable of sustaining flight after liftoff, it is likely that the cascading alerts (the ECAM message and the RETARD alert) and the lack of V-speed callouts eventually led the captain to have a heightened concern for the airplane's state as rotation occurred. FDR data indicate that the captain made erratic pitch inputs after the initial rotation, leading to the nose impacting the runway and the airplane bouncing into the air after the throttle levers had been returned to idle. Airbus simulation of the accident airplane's acceleration, rotation, and pitch response to the cyclic longitudinal inputs demonstrated that the airplane was responding as expected to the control inputs. Collectively, the events before rotation (the incorrect runway programmed in the FMC, the "thrust not set" ECAM message during the takeoff roll, the RETARD alert, and the lack of required V-speeds callouts) should have prompted the flight crew not to proceed with the takeoff roll. The flight crewmembers exhibited a self-induced pressure to continue the takeoff rather than taking the time to ensure the airplane was properly configured. Further, the captain initiated a rejected takeoff after the airplane's speed was beyond V1 and the nosewheel was off the runway when he should have been committed to the takeoff. The flight crewmembers' performance was indicative of poor crew resource management in that they failed to assess their situation when an error was discovered, to request a delayed takeoff, to communicate effectively, and to follow SOPs. Specifically, the captain's decision to abort the takeoff after rotation, the flight crew's failure to verify the correct departure runway before gate departure, and the captain's failure to move the thrust levers to the TO/GA detent in response to the ECAM message were all contrary to the operator's SOPs.
Source: NTSB Report DCA14MA081, p. 2
It used to be a widely accepted practice that your hands should never leave the throttles/power levers/thrust levers during the takeoff. But somewhere along the line most of us adopted the hands off at V1 to drive home the idea that you do not abort above V1. When this change came about, many of us thought it unnecessary. But case study after case study shows the hands off idea is a sound one. When you are startled, your first reaction could be wrong. But in this case, the hands off precaution failed. What many of us need to realize that when something goes wrong, your best first reaction could be to do nothing, give it a second. One of the few exceptions to this is the V1 decision. But we need to discipline ourselves that once the V1 decision is made, as denoted by our hand leaving the thrust levers, that decision has been made.
According to recorded data and interviews with the accident crew, on takeoff the crew received an aural RETARD alert at a speed of about 80 KIAS after setting FLEX thrust. The captain stated that he had never heard an aural RETARD on takeoff, only knew of it on landing, and did not know what it was telling him. He further said that at 86 KIAS when they received the aural RETARD alert, he was not going to reject the takeoff because procedurally they were at high speed, they had no red warning lights, and there was nothing to suggest the need to reject the takeoff.
Source: NTSB Report DCA14MA081, p. 18
This is probably a valid point, in the high speed range perhaps the aural "Retard!" alert was not a reason to abort. (It is debatable, but let's give the captain the benefit of the doubt.) But the 80 knot callout was never made.
- According to the US Airways A319/320/321 Pilot Handbook, Section 2d.6.2 "Go/No Go Concept," to compensate for reaction time, the first officer must call "V1" 5 KIAS before V1, and the captain must recognize the command and respond in a timely manner. The first officer stated that she noticed there were no V-speeds depicted on the PFD at about 120-140 KIAS, and she could not call V1 or VR during the takeoff. She indicated further that she made no other callouts for the takeoff. According to a US Airways A320 check airman, the "80 knot" callout was used to make sure both pilots were in the loop and also as a check for both pilots of all three airspeed indications. The first officer also said she "assumed [the captain] wouldn't continue to takeoff if he did not know the V-speeds." She was not aware of anything that recommended rejecting or continuing a takeoff when there were no V-speeds, and according to her interview, the captain told her "we'll continue and take care of it in the air."
Source: NTSB Report DCA14MA081, p. 21
The captain's "we'll continue" command came considerably later during the takeoff roll.
- An A320 check airman told NTSB investigators that he had never seen anyone take off without V-speeds and that doing so was not trained; if there were no V-speeds displayed, he would expect a crew to reject the takeoff and taxi off the runway. The US Airways Airbus fleet director told NTSB investigators that, in the event a pilot did not have V-speeds displayed for reference, the airline would take that to mean the pilot did not finish the checklist and should not have taken an active runway.
- The US Airways FAA aircrew program manager stated that he had never seen a situation on the line or in the simulator where a pilot initiated a takeoff roll with no visible V-speeds on the PFD. He said that the lack of V-speeds on the PFD during the initial takeoff roll would be consistent with the airline's reject criteria and would probably be a reason not to begin the takeoff roll in the first place since the V-speeds were supposed to be confirmed before takeoff.
Source: NTSB Report DCA14MA081, p. 21
The crew
The captain, age 61, was hired by Piedmont Airlines on March 3, 1986. US Airways (then USAir) purchased Piedmont Airlines in 1987 and merged operations in 1989. His background was all civilian flying, including flight instruction and flying for a commuter airline for about 5 1/2 years before being employed with Piedmont Airlines. The captain estimated his total flying time at 23,800 hours, including about 7,500 hours as pilot-in-command and about 4,500 hours on the A320.
The first officer, age 62, was hired by US Airways as a pilot on March 25, 1999; she had been hired as a flight attendant by Piedmont Airlines in July 1973. She started flying in 1986 and became a certified flight instructor for Piedmont Aviation for several years before getting hired by CCAir (a regional code-sharing partner with US Airways) in 1990. She was furloughed from CCAir for a short time before being recalled in 1991 and flew the Jetstream. She was furloughed from US Airways from March 2, 2002, to April 15, 2007, and was trained on the A320 upon returning from furlough. The first officer estimated her total flying time at 13,000 hours, including about 4,700 hours on the A320.
Source: NTSB Report DCA14MA081, p. 6
Abort Philosophy
- According to the US Airways A319/320/321 PH, Section 2d.6.5 Maneuver, the captain is responsible for calling for and executing a rejected takeoff.
- US Airways trains its captains to have their hand on the thrust levers for takeoff and remove their hand once the V1 callout is made by the first officer. US Airways A319/320/321 Pilot Handbook, Section 2d.6.5 Maneuver, indicates that, when alerted to the non-normal situation before V1, the captain should call "Reject, My Aircraft" while closing the thrust levers, engaging reverse thrust, and immediately applying maximum wheel braking using autobrakes or manual braking.
- According to the US Airways A319/320/321 PH, Section 2d.6.4 Recommended Guidelines, and interviews with US Airways A320 check airmen, below 80 KIAS on takeoff was consider the "low speed regime," and US Airways recommended a rejected takeoff for items such as engine failure, fire or fire warnings, or inability to develop rated takeoff thrust without exceeding engine limits, unusual noise or vibration, tire failure, amber MASTER CAUTION light, abnormally slow acceleration, or the perception the airplane is unsafe or unable to fly. Between 80 KIAS and V1 was considered "high speed regime," and US Airways recommended a rejected takeoff for items such as engine failure, aircraft aural fire warning, or the perception the aircraft is unsafe or unable to fly.
- The US Airways A319/320/321 PH, Section 2d.6.5 Maneuver, states the following:
The captain will make the decision to reject the takeoff and must always be mentally and physically prepared to do so if conditions warrant. He should have his feet in position to apply the brakes and hand ready to retard the thrust levers. If the FO is PF, the captain will replace the FO's hand on the thrust levers after the thrust levers are set in the proper detent. As the aircraft accelerates towards V1, the decision-making process shifts in favor of the "Go" decision.
Source: NTSB Report DCA14MA081, p. 22
The captain said in his statement following the accident that he rejected the takeoff once the airplane became airborne because he "had the perception the aircraft was unsafe to fly and I decided the safest action was to not continue." He stated further that he rotated at about 159 KIAS and when the airplane became airborne, "I felt like the airplane was totally unsafe to fly." He said everything was normal except the chime and RETARD aural alert, and the airplane tracked down the runway normally. He stated that when he rotated, the main landing gear "came off the ground fine and the initial pitch felt fine."
4
Cause
The NTSB probable cause says what happened, not why it happened. We can't get into the heads of these pilots so we cannot produce a cause "beyond a reasonable doubt." But this is not a court of law, it is flight safety where our objective is to prevent recurrence. So allow me to speculate.
While most major airlines have adopted Crew Resource Management (CRM) programs, most also have an entrenched seniority system that places complete command authority with the captain. With time, many captains can go long periods without ever being questioned in the cockpit and this can breed a complacency of many types, including a disregard for aircraft and company Standard Operating Procedures (SOPs). Regular simulator and line checks are designed to prevent this, but at some airlines a captain's evaluation can be little more than a "gentleman's evaluation" at best, a square filler at worst. And even if the evaluation system is on the level, many captains can adopt a split personality about these things: act one way with supervision, another way without. It takes a highly disciplined and professional captain to avoid this.
If an airline, even a CRM-friendly airline, becomes populated with captains who do not react favorably to criticism in the cockpit, fewer and fewer first officers will be willing to offer any. This can turn some first officers into passengers in a pilot's seat.
It appears to me this particular captain had become sloppy in procedure and didn't think twice about violating SOP after SOP. I think his response to the NTSB regarding why he didn't rest his thrust levers to TO/GA in accordance with SOP might typify his attitude. He elected to ignore procedure because there was "no harm" in doing it his way. Had he followed procedure, the annoying "RETARD!" message would have gone away. There is no doubt the repeated "RETARD!" warnings had startled him and there may have been an element of panic. But a captain who had fully embraced SOP would have aborted when it was safe to do so and would have resisted the urge to abort when it was the wrong thing to do. I also thing a more assertive first officer could have knocked some sense into this captain before the situation got out of hand.
The National Transportation Safety Board determines the probable cause(s) of this accident to be: the captain's decision to reject the takeoff after the airplane had rotated. Contributing to the accident was the flight crew's failure to follow standard operating procedures by not verifying that the airplane's flight management computer was properly configured for takeoff and the captain's failure to perform the correct action in response to the electronic centralized aircraft monitoring alert.
Source: NTSB Report DCA14MA081, p. 3
References
(Source material)
NTSB Aviation Accident Final Report, DCA14MA081, Airbus A320-214, N113UW, 03/13/2014.