It is often said that the two most dangerous words in aviation are "watch this." There is no shortage of bad ideas out there but the ones that concern me are old sayings that have a history of being wrong but are still held by some pilots. Let's look at a few.
— James Albright

Updated:
2018-10-20

A low pass by a Falcon 900LX
A common denominator seems to be that some pilots absolutely believe what they are doing is safe, until they end up breaking something. At that point they point the blame to the airplane, their training, or something else. I've had my share of bad ideas over the years. But once I figure that out, I am the first to say, "I screwed up," and then I try to spread the word so nobody else falls for the same stupid idea.
I hope that you don't believe in any of these bad ideas. I have ongoing conversations with a few pilots who disagree with me. Maybe I'm wrong. You be the judge . . .
1 — "Train (in the aircraft) like you fight"
2 — "Never go around beyond the final approach fix with the gear down"
4 — "Any airplane can be flown like any other airplane"
5 — "The mechanic already did the preflight"
6 — "There is nothing better than a visual approach"
7 — "If the approach doesn't exist, build it!"
9 — "I can get more performance from the airplane than the guys who designed it!"

1
"Train (in the aircraft) like you fight"
"Train like you fight, fight like you train" is a sound idea for a military flying unit where your job is to kill people and break things. But when you do that, training losses usually exceed wartime losses. That has been true in the U.S. Air Force and Navy since the dawn of military aviation. But when you aren't fighting a war and when you have simulators, it is a bad idea to play so close to the edge of safety.
My generation of Air Force pilots have been especially guilty of playing too close to the edge in an effort to train others. We had simulators, but the simulators were not very good, we didn't have access to them as much as we needed, and we got bored doing the same thing over and over again. Then one day, somebody had the bright idea to start pulling circuit breakers while flying airplanes.
Case Study: G159 YV-08CP

G159 gear up landing, Simon Bolivar International Airport, Maiqueti, Venezuela, 08-27-1993, (Courtesy Ivan Betancourt)
From a reader: "This G159 landed gear up. The PIC was conducting a command upgrade checkride. They were configured for a flaps 0 landing on runway 09 when ATC instructed them to join right downwind and land on runway 26, a parallel runway (SVMI). The examiner was known to pull CBs and disable warning systems as part of his checkride routine. Well, he disabled the gear horn warning (no idea why he would do such a thing) but when combined with fatigue, distraction, incredible foolishness and over confidence the outcome was predictable."
A Personal Story:
When the 89th Military Airlift Wing flew the Lockheed JetStar (C-140), just about all of the training was conducted "in house" and instructors became creative about how to place their students under stress. The idea was to make the training as difficult as possible so that the mission itself became easy. Fair enough. The JetStar was practically bullet proof, the story goes. In the late eighties the aircraft were replaced with the Gulfstream GIII (C-20), the same cadre of instructors looked at ways to play the same training games. It didn't matter that they had access to very good simulators. So we ended up cutting engines during takeoff, and failing all sorts of systems from before engine start all the way to landing. So we started pulling circuit breakers.
My last job at Andrews was as the Wing's Chief of Safety, while also a qualified C-20 pilot. We were having a rash of aircraft with Electronic Flight Instrument System (EFIS) failures. It seemed curious that the civilian version of the airplane didn't have these problems and that our instructor force delighted in pulling the EFIS circuit breakers to force the student to select alternate instruments or to fly the airplane using standby instruments. When I was appointed as the Wing's Chief of Safety, I managed to convince the wing to place a one month ban on pulling EFIS circuit breakers. To the delight of the maintenance squadrons, our EFIS problems went away. After I left the wing the ban was lifted, the circuit breaker pulling resumed, and so did the EFIS problems.
The aircraft that replaced the C-20 cannot tolerate these kinds of circuit breaker shenanigans so the practice was dropped. (Or so I am told.)
My Take:
Since those days, most manufacturers have become rather explicit about pulling and resetting circuit breakers. To paraphrase a few manufacturers: the circuit breaker is not a switch, don't pull them unless the checklist tells you to, don't reset them without fully considering why they had popped in the first place.
2
"Never go around beyond the final approach fix with the gear down"
Why would a production test pilot make a series of mistakes that a novice pilot would have avoided? Sometimes confidence overpowers caution. Why would a highly experienced combat pilot make a procedural error a moderately experienced Gulfstream pilot would have gotten right? Sometimes non-applicable experience works against you. Why would a pilot trained in the precepts of Crew Resource Management ignore an input from another crewmember that could have prevented the accident in the first place? Sometimes being taught CRM doesn't mean you've fully embraced CRM.
Case Study: G550 N535GA

N535GA aftermath
The hydraulic system that provides pressure for the flaps, ground spoilers, and wheel brakes failed on short final. The copilot said "should we go around to check it out?" To this, the pilot flying said "no . . . we're gonna land cause it's leakin'."
Experienced Gulfstream pilots know the airplane doesn't "sit" on landing with the ground spoilers inoperative and endeavor to fly the airplane onto the runway. This pilot had difficulty getting the airplane onto to the runway and didn't touchdown until 2,048 feet down the runway, leaving 4,453 feet to stop. It then took 8 seconds to lower the nose gear. The pilot deployed the right thrust reverser, but the left was inoperative because of the left hydraulic system failure. The pilots failed to extend the speed brakes. With only 3,000 feet remaining, they discovered their wheel brakes were inoperative. At this point the emergency brakes could have stopped the airplane. The pilot instead attempted to abort the landing and takeoff. Gulfstream tests show this would not have worked. The copilot pulled the throttles back, very likely saving their lives. More about this: Accident Case Study: Gulfstream G550 N535GA.
A Personal Story:
My Boeing 707 squadron in Hawaii had a rash of flap problems which only became apparent after the gear was extended. This is actually a common trait of many airplanes: you can't get that last notch of flaps until the gear is extended. We had a pilot run into this and was told to land at Honolulu International Airport's longest runway, but to remain short of an intersecting runway. The pilot told tower he needed all of the runway and tower said he could either comply or go around. The pilot elected to land. He managed to stop prior to the intersecting runway but all eight main gear tires exploded from the braking effort. The airplane was damaged and the runway was closed.
My take:
I have never been taught it is better to land than go around if I had a problem after the gear was down. I think this is probably true if you are on fire or if something happens but leaves no doubt about the airplane's ability to stop. But if you insist on this idea, I urge you to consider a few exceptions:
- If any system needed to stop the airplane (spoilers, flaps, reversers, brakes, tires, etc.) is impacted.
- If anything happens that invalidates your planned landing performance calculations, such as a smaller flap setting, inoperative spoilers, inoperative reversers, anti-skid system failures, etc.
- If anything happens environmentally that impacts the runway, such as contamination or obstructions.
In other words, there are so many exceptions to this idea of not going around, so as to make it a bad idea.
3
"Watch this!"
There is no shortage of examples of pilots showing off just prior to their deaths. I suppose the classic example is Pinnacle Airlines 3701. But there are so many more.
Case Study: Pinnacle Airlines 3701

Pinnacle Airlines 3701 wreckage,
from NTSB
On October 14, 2004, a Pinnacle Airlines crew flew their Canadair Regional Jet CRJ-200LR on a deadhead leg from Little Rock National Airport, Arkansas (KLIT), destined for Minneapolis-St. Paul International Airport, Minnesota (KMSP). It seemed to them the perfect opportunity to join the rumored “Four One Oh Club,” reserved for the few members of the airline that had ever made it to the aircraft’s service ceiling of 41,000 feet. They made it to that altitude, but they also made the news as two reckless pilots who didn’t understand the aerodynamics of high-altitude flight or, it seems, the basics of how to recover from a stall. For their trouble, they were nominated for the 2004 Darwin Awards, given for stupid acts that serve to “thin the gene pool.”
The airline had flight planned the trip at 33,000 feet with just the two pilots on board. Just five seconds after takeoff the crew began the first of several pitch-up maneuvers that at one point caused stick shaker and pusher activations. These maneuvers included large rudder and aileron inputs and continued through 25,000 feet where their vertical velocity briefly reached 9,000 feet per minute. At this point they asked for and were given clearance to Flight Level 410. When asked about this, the captain told air traffic control, “we don’t have any passengers on board, so we decided to have a little fun and come on up here.” In less than three minutes, the aircraft ran out of speed.
In the next few minutes the crew mishandled several stick shaker and pusher activations with improper stall recovery procedures and continued to increase pitch to the point the aircraft entered an aerodynamic stall. The aircraft rolled sharply, up to 82° of bank, finally forcing the nose down. The crew managed to recover from the upset at 34,000 feet, but not before both engines had flamed out. The crew mishandled the wind milling engine relight procedure, which would have required at least 300 knots. Their speed had been as low as 150 knots and never exceeded 236 knots. Once they descended low enough for an APU-assisted start, both engines were frozen at 0% RPM. With less than a minute to live, the crew made a conscious decision to avoid a housing area, thereby limiting the fatality count to two.
The Pinnacle pilots clearly didn’t understand a fact of life known by most high-altitude pilots: just because you have enough thrust to make it to an altitude doesn’t mean you can hold that altitude. Engine thrust limits and warm outside air temperatures can erode airspeed margins very quickly. Once the aircraft stalled the pilot flying failed to positively break the stall by aggressively lowering the angle of attack. He was, perhaps, attempting to minimize altitude loss as his stall recovery training taught him. Their low speed at high altitude with failed engines produced one unpublicized final surprise. The high-pressure turbines of their engines had close-tolerance seals to improve efficiency. When the engines flamed out, the huge difference in temperatures cause some parts to contract faster than others, causing the engines to seize, a phenomena known as “core lock.” The only way to prevent core lock is to keep the turbines spinning, by windmilling them at a very high airspeed. The crew was never taught this. The appropriate manuals have since been modified to include the immediate action caution: “Failure to maintain positive N2 may preclude a successful relight.”
More about this: Case Study: Pinnacle Airlines 3701.
My take:
There are broader lessons for the entire pilot population, even those not flying jet engines manufactured with the tight tolerances of the CRJ. Chief among these lessons is this: you don’t know everything you need to know when operating outside of “normal” conditions. If you’ve never had the airplane in a regime of flight before, you might not be assured that anyone has. It is in your best interest to get back into the operating envelope as soon as possible.
Case Study: Citation Bravo OK-ACH

Citation OK-ACH (Vaclav Kudela)
On February 14, 2010, a pair of Cessna 550B Citation Bravo pilots were on an empty leg from Praha-Ruzyne International Airport, Czech Republic (LKPR), destined for Karlstad Airport, Sweden (ESOK). The copilot was the more senior of the two and was the Pilot Flying (PF). The pilot in command was the Pilot Monitoring (PM). While the airplane was climbing into the night sky, the PM said, “I didn’t fly night for long time.” The PF asked, “Have you already experienced a roll during night?” She answered, while laughing, “Yes, really.”
A few minutes later, as they were still in the climb to FL 260, the PF rolled the aircraft left and right, perhaps playfully. The PM said, “Let’s go, we are high enough, you nettle me, come on.” The PF said he would wait for a higher altitude. Once at FL 270, the nose was raised to a pitch angle of 14° and rolled to the right. After 4 seconds the aircraft was inverted. In another 4 seconds the aircraft rolled another 90° but its pitch decreased to -85° and the airplane impacted the ground nearly vertically.
Subsequent investigation revealed the pilots had never been trained in aerobatics but had flown aerobatics in the past with other company airplanes. It was a moonless night and the aircraft’s artificial horizon was not designed for inverted flight. Up until the point the roll was initiated, there were no indications of any technical problems.
My take:
As a pilot who has been trained to fly aerobatics, I can’t imagine doing so at night. Over the years I’ve heard stories of pilots who have taken their transport category aircraft into the realm of aerobatic flight and when I protest, they remind me of legendary test pilot Alvin “Tex” Johnston’s barrel roll of a Boeing 707 prototype over Lake Washington on August 7, 1955. Though I am tempted to say, “he was a company test pilot paid to take risks and sell airplanes,” I don’t. I think the better retort is, “two stupid acts don’t make a smart act.”
4
"Any airplane can be flown like any other airplane"
I think we tell ourselves "any airplane can be flown like any other airplane" as a way of saying we don't need to work at relearning when we move from one type to the next. It is even institutionalized by one of the Flight Safety Foundation's Golden Rules: "Automated Aircraft Can Be Flown Like Any Other Aircraft."
Case Study:

N23AC, courtesy Johan Ljunghadl.
This mishap was due to the pilot's inability to maintain directional control in a crosswind during takeoff. The aircraft started to diverge from centerline less than 1,000 feet into the takeoff roll. The airplane departed the paved surface, landing gear and other components separated from the aircraft, the airplane slid on its belly, became airborne momentarily, and came to a rest in a parking lot. Everyone on board was killed.
The NTSB and the world writ large placed emphasis on the position of a switch in the cockpit that links the nose wheel steering to the rudder. The existence of the nosewheel pedals disconnect switch owes to the progression of GIII pilots into the GIV. The older aircraft didn't have a connection between the rudder pedals and the nosewheel steering and Gulfstream wanted to make them comfortable with old techniques in a new airplane. In the GIV and those airplanes that followed, I've yet to see a credible reason to ever disconnect the pedals from the nosewheel steering. But I don't think this had anything at all to do with the crash.
So why did the pilot lose control of the aircraft? The answer was buried in the NTSB Report: "The PIC tended to unload the nose wheel on the G-IV during takeoff to make it easier on the airplane on rough runways."
The Pilot Flying had more propeller time than jet time and was known to lift the nose of the airplane early in an effort to "make it easier on the airplane on rough runways." This is a poor technique in a multi-engine jet. A multi-engine jet will have a large vertical fin and rudder to compensate for the adverse yaw from an engine failure. With or without an engine failure, that large vertical fin acts as a weather vane and tends to turn the aircraft into the wind. The primary responsibility of every pilot is to maintain aircraft control and in a crosswind a tricycle gear airplane — certainly a GIV — needs to have the nose wheel on the runway at least until VMCG.
More about this: Case Study: Gulfstream GIV N23AC.
The winds were 60° off runway heading at 20 gusting to 35 knots. The aircraft was controllable on the ground so long as the nosewheel stayed on the ground until rotation speed, as is the standard operating procedure on that airplane. This pilot caused the crash by using procedures from his light aircraft experience, which were unsafe in this larger, multi-engine jet.
A Personal Story:
When I was a flight examiner in my Air Force EC-135J (Boeing 707) squadron I heard a new copilot showed up who believed the best way to land the airplane was to chop the throttles to idle at 100 feet and then put both hands on the yoke to manage the landing. This actually worked in his previous airplane, the KC-135A. But there were big differences between the KC-135A and the EC-135J. The former had pure turbo jets with a quarter of the spool up from idle time. The latter weighed 50,000 lbs more and tended to drop like a rock at idle power. I took the unusual step of telling the pilot the check ride would be over the second he did that with me on the airplane. (The Lovely Mrs. was too young to attend her husband's funeral.)
My take:
Every change of aircraft should involve an inventory of procedures and techniques to see what works and what doesn't. Your best source of information may be someone who had made the transition before you and has enough experience to have been "bitten" once or twice. But don't rely on just one source. If your favorite Gulfstream pilots tell you the airplane is landed "wing low" in a crosswind, for example, find another source. (More about that, in particular: Crosswind Landing.
5
"The mechanic already did the preflight"
I hear this all the time, and sometimes I hear it during recurrent. It is so obviously wrong, I continue to be surprised when I hear it. Take, for example, the need to check pitot static ports. What can happen? What indeed.
Case Study: Gulfstream GIV N450KK

A close up of the "safety port" (not what Gulfstream calls it), NTSB photo
This accident took place back in April of 2015 and offered a chance for pilots to see just how important a thorough preflight is. But it took the NTSB over two years to write the accident report and they got it terribly wrong. If you believe the report, we are all at the mercy of mud daubers.
The report is so poorly written it is hard to figure out what the crew actually did. It appears to me they didn't follow the checklist at all. But that is just me reading between the lines and putting more credence in the flight data recorder than the report's narrative.
While approaching to start the descent to FXE, at flight level 430, the pilots observed a red "9.8 CABIN DFRN" warning message on the crew advisory system (CAS), indicating a maximum cabin differential pressure of 9.8 pounds per square inch differential (psid) or greater, followed by a red "DOOR MAIN" warning message. According to the digital flight data recorder (DFDR), this was preceded 21 seconds by the illumination of the amber Master Caution switch. The pilots then donned oxygen masks and referenced the airplane's quick reference handbook (QRH) for the emergency checklist. The pilots then heard a loud "bam" sound in the cabin and immediately initiated a descent in accordance with the QRH.
The pilots claimed they opened the cabin pressure outflow valve at this point, but there is no evidence that is true. The "bam" was the internal floor buckling from the over-pressurization. The NTSB says the cabin pressure relief/safety valve failed due to an obstruction of the CPRV static port and "the reason for the initial over-pressurization condition could not be determined." In my view the airplane was heavily damaged by the lack of a proper external preflight, not a mud dauber.
More about this: Case Study: Gulfstream GIV N450KK.
Nobody was killed in this accident, but that wasn't true in another static port accident: Case Study: Aeroperu 603.
A Personal Story:
I have been in few flight departments where this was conventional wisdom: you are wasting your time doing the external preflight. Or that doing the external preflight is nothing more than "eye wash." Years ago we hired a former FlightSafety International instructor who became progressively more lax about the preflight. I once flew three flights where I thought I felt brake oscillations as the flaps or spoilers were selected while I was applying brake pressure. During the next preflight I found one of the hydraulic accumulators was completely depleted and that the accumulator itself was broken. I asked the pilot how it was during the previous preflight. He confessed to have never checked it, he assumed if the accumulator was low we would have gotten a cockpit message. (That is not the case.)
My take:
It is all too easy to assume everything was okay before, so it is going to be okay again. It is especially tempting to think that when the weather is very cold or very hot. But the price of missing things can be very high.
6
"There is nothing better than a visual approach"
I've been hearing this all of my flying career. We want the visual because it is (a) easy and (b) fun. We need to add an item: (c) risky.
It would be tempting to say the biggest concern is landing on the Wrong Airport. But we have come very close to a much worse result.
Case Study: Air Canada 759

Air Canada 759 about to overfly three airliners on a taxiway, NTSB Accident Docket.
- On July 7, 2017, about 2356 Pacific daylight time, Air Canada flight 759 (ACA759), an Airbus A320, Canadian registration C-FKCK, was cleared to land on runway 28R at San Francisco International Airport, San Francisco, California, but instead lined up on parallel taxiway C, where four air carrier airplanes (a Boeing 787 followed by an Airbus A340, another Boeing 787, and a Boeing 737) were awaiting takeoff clearance. ACA759 overflew the first airplane on the taxiway and descended below 100 ft above the ground, and the ACA759 flight crew initiated a go around. The flight was operated under the provisions of 14 Code of Federal Regulations Part 129 as an international scheduled passenger flight from Toronto/Lester B. Pearson International Airport, Toronto, Canada, with 135 passengers and 5 crewmembers on board. Night visual meteorological conditions prevailed at the time of the incident. The airplane was not damaged, and no injuries were reported.
- At 2355:45, the pilot of ACA759 transmitted to the LC/CIC controller, “Just want to confirm, this is Air Canada 759, we see some lights on the runway there, across the runway. Can you confirm we’re cleared to land?”
- At 2355:52, the LC/CIC controller responded, “...confirmed cleared to land runway 28 right. There's no one on runway 28 right but you.” The pilot of ACA759 replied, “OK, Air Canada 759.”
- [The LC/CIC controller said in his interview that he had just visually scanned the runways from departure end to approach end when ACA759 asked for confirmation on the landing clearance. He then checked the radar display 7 and the ASSC8 display (airport surface surveillance capability), and rescanned runway 28R before advising the pilot that runway 28R was clear. He looked at the ASSC display and saw the data symbol for ACA759 just right of centerline, and the bars on the runway were up [indicating the runway was clear]. He said that the position of ACA759 (data symbol) on the ASSC was normal for the Bridge visual approach.]
- At 2355:59, a transmission was broadcasted over the local control frequency, “where is that guy going?” Three seconds later, another transmission was broadcasted, “He’s on the taxiway.” [Crew statements from United Airlines flight 1 (UAL) indicated they made those transmissions]
- At 2356:09, the LC/CIC controller instructed ACA759 to go around. The pilot acknowledged that he was going around. The LC/CIC controller advised the pilot that he appeared to have been lined up for taxiway C.
Source: NTSB Docket
The NTSB analyzed the lowest point of Air Canada 759 and determined they came within 13.5 feet of an A340's tail on the taxiway. There was an operating ILS to Runway 28R as well as an RNAV(GPS) available to back up the visual approach. There were several complicating factors to this event, not the least of which was crew fatigue and an impossible to read list of NOTAMs. The fact Runway 28L was closed was item 45 in a list of 50. The aircraft's localizer was not tuned to the 28R frequency.
More about this: Air Canada 759.
A Personal Story:
My Air Force Boeing 747 squadron had a pilot nearly land on a runway too small to support it and a friend of mine actually did that in an Atlas Air Boeing 747. Read about both of those incidents: Stories: The Wrong Airport (1986).
My take:
Even if you think flying your jet without reference to an instrument approach is a sign of superior airmanship and superior fun, you should consider the great number of superior airmen who managed to line up on the wrong slab of concrete. You should always use all situational awareness tools available to you and the best of these may be the trusty old ILS. But these days with GPS you need never make a visual approach without an accurate back up. More about this: Business & Commercial Magazine "Wrong Airport" (January 2018).
7
"If the approach doesn't exist, build it!"
In the previous section we have pilots who want only to fly visual approaches but we have the opposite here, pilots that cannot fly without some kind of course guidance, even if it means building that guidance against regulatory restrictions. Can you build your own approach? Yes. Should you? There are so many ways to get it wrong that the answer has to be no.
Case Study: Air Blue 202

Air Blue 202, Pakistan Civil Aviation Safety Investigation Report, cover page.
The captain of this Airbus A321 was worried about having to circle at Chaklala International Airport, Islamabad, Pakistan. The weather was just good enough for the left pattern. For some unknown reason, the captain preferred the right pattern and had the first officer build that into the FMS. Tower denied their request for a right pattern several times, due to low clouds on that side of the airport. The captain commanded the right turn for the left pattern by selecting heading mode. He then heard a competing airline had just landed, flying the left pattern. The accident report said that "put the Captain under further pressure to ensure a landing at Islamabad under any circumstances."
The report speculates that the captain decided to fly a right pattern at this point by saying he was "going for NAV" but neglected to select the mode. The aircraft remained in heading mode even as the crew noted passage of the waypoints they had built. The crew looked in vain for the airport (perhaps looking to the right when it was to the left) until about several miles north of the airport, at which time NAV was selected. The radar controller instructed them to turn left. The captain said he was turning left, but he was moving the heading bug while the autopilot was still in NAV mode. They hit the terrain a few seconds later and all 152 persons on board were killed.
There was much more going on in the cockpit, not the least of which was a break down in CRM. I think the Pakistani report suffers in translation so the facts are not explicitly laid out. The ad hoc approach they had built in the FMS didn't cause the crash but selecting the approach after they became lost delayed their recognition of a need to go missed approach before they impacted the terrain.
More about this: Case Study: Air Blue 202
A Personal Story:
I went to Gulfstream GV initial training in early 2006 and was warned that Savannah FlightSafety International instructors were teaching pilots to build circling approaches in the FMS and were, in fact, insisting on it as a condition of passing a check ride. I was a check airman for TAG Aviation and AMI Jet Charter at the time. I complied with their wishes but turned in a massive critique with this: "The GV Flight Management System’s inability to fly circling approaches using FMS data is certainly an inconvenience to those of us coming from Collins and other FMS makers. That inconvenience does not authorize us to violate the limitations and procedures placed on us by the aircraft manufacturer and the FAA. FlightSafety Savannah should be teaching ways to live with the restrictions and not encouraging wholesale violation."
To their credit, the Savannah training center stopped the practice of building approaches in the GV FMS.
My take:
There are times when flying what the Honeywell world calls a PBD (Place / Bearing / Distance) waypoint helps situational awareness and should be encouraged. But you should never fly such a waypoint as a means of getting down to instrument minimums or navigating through terrain. The practice is prohibited by several FAA advisory circulars and orders. (See AC 90-100A ¶ 10.b.(5) for one example) Besides, it is dangerous.
8
"callouts are for newbs"
I have been in social settings where the topic de hour was how some pilots took themselves too seriously (perhaps it was an intended jab at me) or, on the other side of the debate, there was far too much chatter in the cockpit and wouldn't it be best if nothing was said at all? I like a quiet cockpit but I also like standard callouts.
Case Study: Corporate Airlines 5966
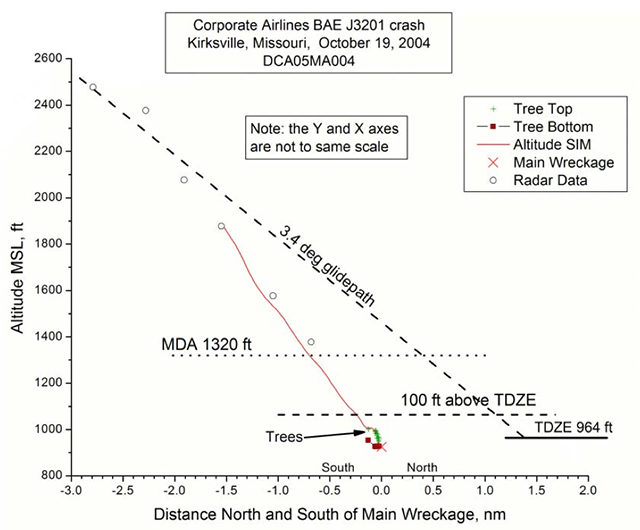
NTSB AAR 06/01, figure 6.
This aircraft was technology poor, but they had what they needed to compute a visual descent point and the techniques to do so were well known at the time. The crew's joking banter prior to the instrument approach may appear harmless, but it sets the wrong tone for the serious work ahead of them. Finally, the first officer missed several opportunities to call for a go around when he lost sight of the runway below the minimum descent altitude. One of the ironies of this mishap is that 28 minutes before their deaths, both pilots were talking about hating pilots who "take themselves too serious." In the end, they didn't take what they were doing seriously enough:
- 1909:30 HOT-1 gotta have fun.
- 1909:31 HOT-2 that's truth man. gotta have the fun.
- 1909:35 HOT-1 too many of these # take themselves way too serious, in this job. I hate it, I've flown with them and it sucks. a month of # agony.
- 1909:47 HOT-1 all you wanna do is strangle the ## when you get on the ground.
- 1909:50 HOT-2 oh'.,.. @ [sound of laughter]
- 1909:52 HOT-1 oh *, yeah, oh well, he was one but I didn't, I didn't have to fly with him that much 'cause....
- 1909:56 HOT-2 I know.
- 1909:57 HOT-1 it was kinda a fluke. but uh, some of the guys that aren't here any more you wanted to just # kick 'em in the #. lighten the # up #.
The pilots failed to make several mandatory callouts, any one of which could have changed the outcome. (15 of 17 on board killed.) For more about this: Case Study: Corporate Airlines 5966.
My take:
When it comes to callouts, there are as many standard operating procedures as there are operators. The important thing is to be consistent: callouts.
9
"I can get more performance from the airplane than the guys who designed it!"
When I was in the ratings chase, flying my trusty T-37, I often stretched the range string to its maximum. A training sortie was usually 1.3 hours, we could get 2.0 out of the airplane. I've done 16 in the Boeing 707 and 20 in the Boeing 747. But those included multiple air refuelings. I've done a 10.0 in the G450 and 14.5 in the GV. But in all of those cases, you could rebuild the flight using the AFM performance charts.
If you are doing better than your charts, you are probably doing something wrong.
Case Study: TWA 841
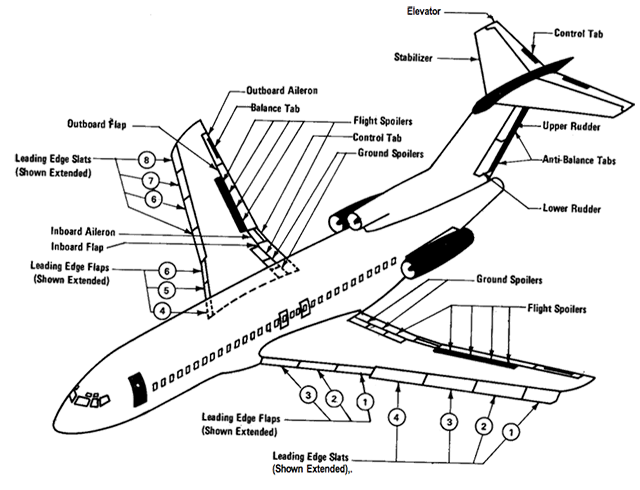
B-727 Flight Control System,
from NTSB-AAR-81-08, figure 1.
The NTSB report looks pretty well thought out but there remains a conspiracy theory out there that Boeing tried to cover up a known problem with the Boeing 727 leading edge slat system at the cost of a good airline pilot's career. The NTSB was very careful in its choice of words but the talk among 727 and TWA pilots at the time was this:
- The trailing edge flaps on the Boeing 727 extend aft a great deal before they extend down. If it were not for the automatic deployment of the leading edge slats, the first notch of flaps would turn the wing into one that produces more lift. (Greater span with very little change in camber.)
- There was a belief among some Boeing 727 pilots that you could increase the airplane's speed by pulling the circuit breakers on the leading edge slats and extending the trailing edge flaps to their first notch.
- The mishap pilots did just this while the flight engineer was aft using the lavatory. When the engineer returned to the cockpit he noticed the popped circuit breakers and reset them, causing the leading edge slats to extend.
- This caused the buzzing sensation the captain noted. When he retracted the flaps the No. 7 leading edge slat failed to retract, causing the subsequent roll.
I think that is probably what happened. More about this: Case Study: TWA 841.
A Personal Story:
When I started flying the Challenger 604 it was a fairly new airplane. But variants of the Challenger 600 and on had been around for quite a while. We had several pilots in our flight department who had been flying one form of Challenger for ten years or more. While the book called for a takeoff rotation rate of 3° per second to a pitch of 14° (two engine) or 10° (single engine), it seemed none of our "experienced" Challenger pilots did that. Half would grab the yoke and haul it up as fast as they could. The other half would use a good rate but never to the required pitch. Everyone had a reason they knew better than Canadair, the manufacturer. Then, in October of 2000, a Canadair test pilot crashed an airplane on takeoff, killing himself and two others. Though it took years to find out why the crash occurred, we eventually found out most of Canadair's production pilots were using the haul the yoke back technique.
My take:
The manufacturer has hundreds and even thousands of hours in the certification process to explore the airplane's envelope. It is in their financial interest to get the most performance out of the airplane as is safely possible. They are doing this with highly experienced pilots backed up by teams of engineers. If you think you've come up with a better way to fly the airplane, you are probably wrong.
10
Are "bad ideas" in the eye of the beholder?
I once heard of a pilot who swore you could increase an airplane's en route speed by over-pressurizing it in a tailwind (to increase the aircraft's cross section and therefore the "push" it got from the wind, or under-pressurizing it in a headwind (to decrease the aircraft's cross section and therefore the resistance it got from the wind). I am positive that person finished his or her flying career believing that.
I think one of the finest attributes in a professional pilot is humility: the knowledge that you cannot know it all, can always learn, and have to be aware of the fact you may someday find yourself in uncharted territory. The best way to avoid that uncharted territory is to stick to known procedures (which produce known outcomes).
References
(Source material)
Advisory Circular 90-100A, U.S. Terminal and En Route Area Navigation (RNAV) Operations, Change 2, 4/14/15, U.S. Department of Transportation
Flight Safety Foundation ALAR Briefing Note 1.3 - Golden Rules
NTSB Accident Docket, DCA17IA1148, Air Canada 759, Performance Study
NTSB Accident Docket, ERA15LA328, N450KK
NTSB Accident Narrative, ERA15LA328, N450KK
NTSB Aircraft Accident Report, AAR-06/01, Collision with Trees and Crash Short of the Runway, Corporate Airlines Flight 5966, BAE Systems BAE-J3201, N875JX, Kirksville, Missouri, October 19, 2004
NTSB Aircraft Accident Report, AAR-07/01, Crash of Pinnacle Airlines Flight 3701 Bombardier CL-600-2B19, N8396A, Jefferson City, Missouri October 14, 2004
NTSB Aircraft Accident Report, AAR-07/06, Runway Overrun and Collision, Southwest Airlines Flight 1248, Boeing 737-7H4, N471WN, Chicago Midway International Airport, Chicago, Illinois, December 8, 2005
NTSB Aircraft Accident Report, AAR-81-08, Trans World Airlines, Inc., Boeing 727-31, N840TW, Near Saginaw, Michigan, April 4, 1979, National Transportation Safety Board, June 9, 1981
NTSB Aircraft Accident Summary, CHI97MA017, Gulfstream GIV, N23AC, October 30, 1996
Pakistan Civil Aviation Authority Safety Investigation Board, Air Blue Flight ABQ-202 REG AP-BJB Pakistan Crashed on 28 July 2010 at Margalla Hills, Islamabad